WingRight
Public Policy
Counterintuitive abortion report
Legalize arbitrary homicide to decrease arbitrary homicide? Talk about counterintuitive!
I enjoy debating bioethics and politics online because it encourages me to think, research and tighten my arguments. I spend at least part of each day explaining and advocating for the protection of human rights, especially the right to life, or the right not to be killed. I’m not only trying to convince the people engaged in the conversation, but the “lurkers” who read but don’t post.
I endeavor to read and evaluate as many as possible of the sources and references that are used to counter my arguments. I learn and hope to be a better debater that way.
During an one such debate, I was referred to a 2020 article in the journal Lancet, “Unintended pregnancy and abortion by income, region, and the legal status of abortion: estimates from a comprehensive model for 1990–2019,” that supposedly gave proof that abortion restrictions result in higher rates of abortion.
The report proves that statistics can be manipulated based on estimates which are actually Wild-Assed Guesses. Working from an estimated 73.3 million abortions per year worldwide, the authors admit that virtually all of the data are “estimates” rather than actual numbers.
But, to strengthen their model, they threw out 62% of women at reproductive age because data from China & India, where abortion is broadly legal, “skewed” their numbers.
Besides the fact that it would be useful to know how they determine the number of illegal abortions in a country, the “findings” are reported by region & broad income. (And in a cluttered pdf at https://www.thelancet.com/cms/10.1016/S2214-109X(20)30315-6/attachment/d4652ad7-9ace-425e-b907-7060ff71982f/mmc1.pdf )
Look at the Caribbean countries where countries with just about every possible combination of restrictions & income level are lumped together. ( And Cuba is reported as upper middle income.)

Which might or might not explain,
…..
“Among middle-income and low-income countries, there was not a clear relationship between legal restrictions and abortion rates, or the proportion of unintended pregnancies ending in abortion.”
And,
“2015–19, low-income countries had the highest unintended pregnancy rate and the lowest proportion of unintended pregnancies ending in abortion.”
If we accept the WAG numbers that the authors admit are higher than those of other researchers, there is an indication that lower income regions have more pregnancies the authors categorize as “unintended.” And, if a country starts out at an abortion rate of 30, increasing to 39 gives a higher percentage change than countries that start at 61 & go to 70.

At least the headings in the Summary are semi-truthful: “findings” & “Interpretation.” But the data doesn’t indicate that restrictions result in more abortions.
Afghanistan: Read this
This is the best, most comprehensive article I’ve read about the events in Afghanistan.
“Calls for air support went unheeded, because America had pulled the maintenance capability of the very aircraft that would have responded. There was no help coming.” (Emphasis mine, BBN)
The US not only withdrew our 2500 troops from Bagram Air Base, the Biden Administration banned non-military contractors from providing technical support – repairs as well as routine maintenance – for the aircraft that the Afghanistan military needed.
Conversation with January 6 protester
“Not one person charged with insurrection!” (January 6) Kash Kelly
While it’s up, Live stream phone call with one of the men in the DC jail, held without bond, after being arrested after January 6, joined by the “Lego guy.”
Kash asks about the magnetic locks on the Capitol.
Tells about the threats of increased charges if he won’t plead guilty.
Points out that the guillotine was erected, recorded, then dismantled before Kash left the Capitol.
The contemporeneous videos have been removed from the day of January 6, but the ones I saw that day supported what is being said here.
Edited to add supporting evidence:
The model of the Capitol that the “Lego man” owned was loose, still in the box, not fully constructed as originally reported by the FBI. https://nypost.com/2021/07/12/capitol-lego-set-seized-from-rioter-in-box-unassembled/
Video made by Kash Kelly and the Change makers just before January 6th, discussing plans for trip to Washington, DC. (Some profanity.)
Discussion about false stories about Mr. Kelly.
Normal & reality: a proposed definition for discussion
On one of the Facebook groups I follow, the conversation about the recent Arkansas law protecting conscience was diverted from the law itself by a sensational headline that reflected only the worst accusations of opponents & the reactions of group members to that headline.
During the conversation, I was questioned about my use of the term “normal” for healthy bodily functions. At the least, “normal” is that which doesn’t itself injure tissues & organs and doesn’t require technological intervention to produce or to prevent morbidity & mortality.
We are hearing & reading about demands that legitimate research results should be suppressed, watching physicians and scientists who express heterodox opinions be censored. Then we’re told that there’s a “consensus,” since none of the “objectionable” research is published, much less popularized, and the outliers are demonetized and covered with warning boxes.
Science isn’t a “consensus.” In science, true hypotheses are testable, with valid results capable of being confirmed by different observers under similar conditions in different labs.
That’s also a good definition of reality or “normal.” One that could be applicable to medical subjects like COVID or vaccines, as well as social and legal matters.
We’re being manipulated for reasons that have nothing to do with actual health, physical or mental. I can’t fathom a reasonable explanation. It looks like an exertion of power – social, financial, then legal.
Patients won’t be helped at all by forcing moral injury by requiring medical professionals to act against their conscience and we all lose when rational discussion is suppressed in the public sphere.
Planned Parenthood’s “Watchlist,” false report about pro-life activists to local police
LiveAction reports that Planned Parenthood sent “watchlist” to Lubbock police before the January March for Life, including photos and
date if birth, other personal informatiion, and designating some of the men and women as “aggressive.”
Apparently, some”central” office of PP made up the list, which makes is wonder how many other local police departments received such lists & what they’ve done with them.
What did PP hope to achieve? Threats against activists by police? Before a pro-life event?
Reporting people who have not committed crimes to the police goes beyond “cancel culture.” Isn’t there a law against false reporting in Texas?
Why Georgia matters
Even failed “progressive” actions by US legislators are rarely, if ever, reversed. Often, they enable broader progressive changes.

As I write this, it’s nine days after the 2020 election and we still don’t know who will be inaugurated as President of the United States. In spite of the precipitous “calling” of the election by the AP an other media for Joe Biden, the actual result is not a given due to close votes in several States. Lawsuits and recounts will likely play out at least until the day of the Electoral College vote, December 14, 2020, if not beyond.
Georgia officials have announced that they will conduct a recount and audit of the vote in that State because the difference in the Presidential election votes is about 0.2%. There’s a chance that the State will determine who will be sworn in on January 20, 2021.
But the biggest impact for the State may be as a result of another election. (Or, technically, two elections.)
On January 5, 2021, the State of Georgia will hold a run off election to determine both of their Senators. Currently, it appears that both races can be handily won by the Republicans if they turn out as they did on November 3, 2020.

(Each race had several candidates and Georgia requires a majority to win. Republican John Purdue beat Democrat Jon Ossof 49.7% to 48%.

While Republican Kelly Loeffler only received 25.9% of the vote in the Special Election compared to the 39.2% won by Democrat Raphael Warnock, the other Republicans in the race bled off Loeffler’s votes have endorsed her, including Doug Collins, who had 19.9% of the vote.)
In the event that Joe Biden wins the Presidential election each of us, regardless of Party affiliation, should ask ourselves whether the current crop of Democrats can govern without turning our Nation over to the chaos that is the status quo in many of the cities they already govern.
In addition, it’s imperative to remember the consequences of compromises and the influence of the Left on policies of the future.
Take an example from my profession: 1993’s “HillaryCare” debacle. Hillary Clinton’s plan to centralize health care to impose universal, single-payer government financed health insurance failed due to closed door meetings and a chaotic lack of political planning. It still resulted in SCHIP, HIPAA, the Balanced Budget Act of 1997 that removed all privacy from medical records and forced utilization of mid-level medical personnel as employees of “providers,” the ridiculous idea that cutting numbers of physicians by restrictions on funding for residencies would save money for Medicare, and ultimately, ObamaCare.
The Republicans have already won 50 seats, at least, but that is no majority and ties would be settled by the vote of the “President of the Senate,” the Vice President of the United States. In the event that Biden is the final winner of the Presidency, those ties would go to Kamala Harris – or her VP after Joe resigns or is unseated.
It’s a cliché that we’re likely to hear slot in the next 2 months, but do keep Georgia on your mind.
Dueling Statements by “Experts:” More COVID-19 politics
Say her name: Jennifer Long, murder victim

Jennifer, 16 yo
This 2001 article about the 1998 kidnapping, rape, murder by stabbing, and dismemberment of 16 year old Jennifer Long takes my sympathy away.
SCOTUS redefines words. Again. (Say goodbye to single sex sports & spaces)
There’s a right way and a wrong way to change a law. The Constitution doesn’t provide that the Courts make the big decisions, leaving the inconsequential matters to Congress. And yet, nominally “textualist” Supreme Court Justices Gorsuch and Roberts joined with the”living document” Progressives to do it the wrong way.
Gorsuch wrote the majority opinion in Bostick v. Clayton County and got at least two points right:
- “When the express terms of a statute give us one answer and the extratextual considerations suggest another, it’s no contest. Only the written word is the law, and all persons are entitled to its benefit.” and,
- There’s no way that the 1964 Congress would have intended for the word “sex” to include sexual orientation or gender identity.
In his 37 page argument, Gorsuch stuffed and fluffed strawman after strawman to fit an extratextual interpretation of “because of …sex” into the redefinition of “sex.” As noted in the dissents by Justices Alito & Kavenaugh, his is a redefinition that wasn’t even attempted when SCOTUS redefined “marriage” in Obergefeld.
In other words, as Justice Alito wrote in his dissent, Gorsuch and the majority “legislated.”
I agree that this law needed changing to give more protection to employees in the public market place. Congress should have been encouraged to work out those protections, while also preserving religious freedoms and single-sex spaces and even women-only sports. I can’t help but wonder whether – perhaps – both political Parties took a dive, hoping the Supreme Court would do exactly what they did.
And the Country will witness lawsuits, year after year, that might have been averted.
In the meantime, though, I’ll bet Senator Chuck Schumer feels caught in a whirlwind of his own. What price, now, Chuck?
Don’t eat the COVID-19 (Coronavirus)
The good news is that we were warned and it’s Spring, not Winter. (And we don’t routinely greet acquaintances with real kisses in the US.)
The really good news is that you aren’t helpless.
Chances are, most of the people who get sick picked the germs up with their hands and put them in their mouth, nose or eyes. (Gross, I know, but, trust me, I’m a doctor and a mother. I can be more gross than that when I want to get your attention.)
I tend to be a skeptic about panics, and so much of the news coverage about coronavirus is political hyperbole, but … I’m reading some worrisome stories from doctors dealing with the outbreak of COVID-19 in Italy.
Don’t panic, and don’t share! The coronavirus is spread by particles, droplets that have to enter your body by way of your nose, mouth or eyes. While it’s possible that someone might infect you by sneezing or coughing in your face, most viral infections are spread because of poor personal hygiene.
Virtually no one is immune to this coronavirus and we won’t have a vaccine for months, so people are panicking. I’m not, and here are some reasons why:
The US isn’t Italy. For one thing, we have a younger population. And, although the Lombardy region in Italy is modern and advanced, we have a higher intensive care capacity.
After all, we easily absorb the burden of influenza: up to 49 million infections, half a million hospitalizations, and 50,000 deaths every year due to influenza and hardly anyone even notices.
And we’ve had more warning than they did.
Here’s how fast influenza spreads each year in the US. If we don’t practice excellent self- protection, it’s a preview of how fast COVID-19 could spread.

Confirmed hospitalization history for Influenza in the US. Red = 2019-20, Orange =2017-2018
What’s the rate of spread of influenza in the US each year? This year? The graph above shows the historic rates of confirmed hospitalizations in the US. The red line is this year and reflects just over 16,000 patients, so far. The bright orange at the top is 2017, when we had a poorly matched vaccine.
There have been 200,000+ positive influenza tests reported to the CDC this year, 16,000 hospitalizations, and 136 pediatric flu deaths – not elderly patients with chronic diseases – this year.
We call it “seasonal” influenza for a reason. People tend to share the virus more in winter because of Thanksgiving and Christmas gatherings (and travel) and because children are in school. Sharing germs.
The coronavirus cases in the US sometimes have unknown “patient 1,” but the bulk have all involved clusters of patients with known physical and/or close contact with someone who was sick. The deaths have mainly been patients in one nursing home and a (different) hospital. In these sites, sick people were exposed to the droplets much more than you or I might be, because medical treatment accidentally aerosolized secretions.
COVID-19 symptoms are a fever over 100.5, a dry cough, and, for some, rapid onset of trouble breathing. Ther might be a runny nose or diarrhea, but there isn’t vomiting.
Use common sense and easy-to-achieve precautions. Wash your hands, don’t touch your face (eyes, nose, mouth), stay out of crowds, kindly and gently use what influence you have to encourage others to do the same.
If you get a fever, don’t go to the ER unless you are having trouble breathing. Call your doctor, and “self-quarantine.”
Most of all, Don’t share your germs and don’t pick up others’ viruses and put them in your body.
(Comments are closed. Please comment on my Facebook page.)
Doing to, not for (Baby Tinslee & TADA)
“We’re doing things to her. Not for her.” (Wini King, spokesperson for Cook’s Children’s Hospital, January 3, 2020) This may be the best description of a very sad case.
Tinslee Lewis was born prematurely on February 1, 2019, with severe heart and lung defects. She had cardiogenic shock and was admitted to the Cardiac ICU at Cook’s Children’s Hospital immediately. ♡(See Cardiac Pathology ♡below.)
Even after three open heart surgeries, a fourth to close her sternum, a short time on ECMO (essentially, heart-lung bypass) and constant ventilator since July, of 2019, Tinslee’s enlarged heart and small, damaged lungs can’t keep up with the necessary blood circulation and exchange of oxygen and carbon dioxide, even with the assistance of multiple blood pressure medicines, diuretics and the ventilator on high, except when she’s still and quiet with the help of sedating and paralyzing drugs.
In response to a lawsuit against Cook’s Children’s Hospital, where Tinslee has been in the CICU since birth, Tinslee’s medical records were submitted to the Court. I’ve been able to review approximately 200 pages that are now public record, describing the constant, repetitive interventions necessary to keep Tinslee alive on the ventilator.
Tinslee’s doctors (and, the notes show, the nurses and staff) believe that they are being forced to cause Tinslee pain and suffering, while keeping her paralyzed and sedated. They report increasing difficulty with managing the ventilator so that her damaged heart & lungs can maintain oxygenation. She requires repetitive heart, lung and blood tests to guide adjustment of meds & treatments and has had several infections requiring treatment. In contrast to my earlier presumption, the notes in the records show that the ventilator and all its required meds and manipulations are indeed causing undesired problems, including fluid overload, infections and cardiopulmonary distress, in addition to her underlying lung disease. Even the baby’s growth, something we usually celebrate, increases her risk of cardiopulmonary insufficiency.
Those records also contain notes from many attempts to explain and council Trinity Lewis, Tinslee’s mother, about her baby’s underlying problems and prognosis and the reasoning behind, in contrast to some past media reports.
Ignoring the fact that doctors, not hospitals, practice medicine in Texas, Texas Right to Life Lawyer Joe Nixon is quoted, claiming that the “hospital ” has decided to withdraw treatment. Texas Attorney General, Ken Paxton, is shown to have Tweeted that the problem is a “legal issue,” rather than an ethics and justice matter of forcing doctors (and by their orders, nurses and other staff) to cause pain and suffering for a little girl who is dying as her body fails to heal, in spite of every intervention possible.
Many people, out of compassion, object that “the family ” should decide when to withdraw life support. Yet, the family members aren’t watching the oxygen levels drop while they rinse Tinslee’s airways with a bicarbonate solution to keep her lungs clear. And it’s certainly not the lawyers that are probing, injecting, measuring and adjusting constant, innumerable hourly interventions done to a baby who must be sedated and paralyzed to prevent cardiac and respiratory distress.
In spite of the diligent complicated interventions and care of the doctors and nurses at Cook’s, there have been comments in blogs and social media that the “hospital” wants to “kill” Tinslee. Startlingly, AG Paxton called the latest Court ordered, indefinite hold on removal of life support a “Stay,” as though the doctors, not her multiple medical problems, would kill Tinslee. He also misrepresents the process that Cook’s Children’s Hospital and Tinslee’s doctors followed,
“The statute fails to require that physicians provide an explanation of why they refused life-sustaining treatment and provide the patient’s family with adequate notice and opportunity to argue their position prior to the committee reaching a decision, effectively allowing the government to deny an individual’s right to his or her own life and to do so without due process.”
In fact, though, it is the lawyers, particularly at Texas Right to Life, who are turning a little girl’s tragedy into a continuation of their legal battle against the Texas Advance Directive Act. I’ve covered the benefits of and the struggle to improve the Act – repeatedly blocked by TRTL and their lawyers – for years on both WingRight.org and Lifeethics.org
The Act, TADA, was hammered out in 1999 by a group of stakeholders including patient and disability advocates, hospitals, doctors, ethicists and lawyers. Texas’ prolife organizations, including TRTL and the organization for which I served on the Board of Directors for 15 years, Texas Alliance for Life, and for whom I wrote this essay.
Briefly, TADA allows a balance and legal options when there’s a difference in opinion between a patient’s desire for a given treatment and the medical judgment (a combination of education, experience, and the standard of care) of the doctors who are tasked with the most difficult medical and surgical cases.
I’ll admit that it’s my opinion – and only my opinion – that the lawyers hate that TADA provides a safe haven from lawsuits if doctors follow the law (!). I slowly came to this conclusion over the years because at virtually every Legislative hearing and stakeholders’ meeting about any changes to the Act, the lawyers bemoan the fact that doctors don’t have to go to court over each of these cases and that they face no legal penalty or “liability.”
Poor Tinslee Lewis will most likely never leave the hospital alive. Disease and death don’t respect “due process,” but, they are predictable and an inevitable part of life. Hopefully, we will see her mother and those who love her come to find peace with her death, celebrating the time they’ve had to be with her, especially these last 2 months. However, I fear that the lawsuits will continue for years, adding to their grief.
Edited 1/19/2020 for a typographical error: in the secondparagraph, “cardiogenic” replaced “carcinogenic.” BBN
♡Ebstein Anomaly – Cardiac Pathology 101, about as simple as I can make it (and understand, too);

(Thanks to Mayo Clinic)
Babies born with Ebstein Anomaly have a malformed right and atrium and ventricle and misplaced (tricuspid) valves between the right sided ventricle and atrium. The larger right ventricle can’t pump efficiently.
In addition, the blood the right ventricle tries to pump into the lungs leaks/flows/churns (risking blood clots) back into the right atrium, which grows even bigger, with even thicker walls. The ventricle also grows bigger. When the muscle fibers of the chamber walls get stretched apart enough, they are less inefficient. (Think of two hands gripping at the fingers. The farther out the grip, palm > 1st joint > fingertips, the less strength and pull on the opposite hand.) (For the geeks: Frank-Starling law.
The lungs aren’t efficiently filled with blood, they don’t expand, the pressure builds up in them and efficient exchange of gasses doesn’t take place.
In the meantime, the blood backs up in the body, the liver, kidneys and extremities & eventually the left side of the heart, which can hypertrophy , too.
The enlarged heart puts pressure on the lungs and nearby soft tissue, including the blood vessels coming to the heart.
The combination of leaking high pressure blood vessels and the body’s increasing fluid in order to try to pump what oxygen there is, leads to edema or swelling of the body.
Sometimes, the fetal atrial-septal defect stays open, allowing mixing of the un-oxygenated blood from the right, with the oxygenated blood. This malfunction can help, temporarily.
With the high pressure, poor flow, and actual physical damage due to the mass of the heart, none of the organs can function well. Increased activity, stress, and growth will increase the demand for oxygen, kidney & lung function.
Eat the Rich (with the rest of us for desert)

Dems used to just act as though government owns your current and future earnings. Now, they want to know the value of your wedding ring, grandma’s China, the homestead, & your golden parachute. The plan is to tax them *every year* until you have to sell them (to them?) to pay those taxes.
- A wealth tax like the one proposed by presidential candidate Sen. Elizabeth Warren would make ultra-wealthy Americans pay the federal government a small percentage of their net worth each year.
- Sen. Bernie Sanders released his own proposal for a wealth tax on September 24 that his campaign claims would cause “the wealth of billionaires would be cut in half over 15 years.”
Suuure it is. That’s what they said about the income tax in 1913. (and you can keep your doctor, too.)
By 1918, the highest tax rate went from 1% to 67%, 77% in 1918. The lowest on incomes less than $4000, went from 0% to 6%.
Yes, in a (coco)nut shell, that is it. If you want the tax break, all you have to do is abandon everything you own, book a flight and never return, or at least not that much anyway.“ (HT: The Points Guy)
If you denounce your citizenship, you may be liable to an “Exit tax” calculated as though you sold everything you own on the day you “expatriate.” And you can’t get your citizenship back.
So, what we have is a bunch of 70 year olds who have enjoyed their wealth and some 20- to 30-somethings who don’t want to pay their student loans and don’t really want to work hard enough to accumulate wealth on their own.
Eat the Rich. It’s a thing.
Nite: comments disabled. Please comment on my Facebook page.
Texas Governor Abbott on “Suspicious Activity”
Texas’ Governor Greg Abbott ( @GovAbbott ) isn’t trying to change Texas law with last week’s Executive Order – in contrast to the claims I’ve seen on my Facebook news feed.
Instead, he called for law enforcement agencies under the executive branch to establish policies and training, and financial incentives to encourage “improving reporting channels and closing ‘information gaps’ when members of the public or law enforcement agencies worry that a person might be a threat to commit violence.“
The last three mass shootings in Texas tell us that we need to improve how our law enforcement and agencies follow current law on following up on reports and investigations.
The Sutherland Springs Church shooter in South Texas should have been rejected at point of sale background check because of his prior conviction and incarceration for domestic violence crimes while in the military. Unfortunately, he was never reported to the Federal database. (And so, Texas law probably couldn’t have made any difference.)
However, the Odessa shooter threatened and brandished a weapon at his neighbor, but local Law Enforcement Officers didn’t follow up because his house wasn’t on their GPS maps and was difficult to find!
The El Paso shooter’s mother tried to report him, but the LEO who spoke to her on the phone dismissed her concerns. No record of the call was made, according to the Allen police department.
I’m not sure that current laws would have (or should have) allowed any action against the (future) shooter by authorities, but it looks like that question and reporting procedures are what Governor Abbott wants clarified. From the Executive Order:
“”Within thirty days of this order, the Texas Department of Public Safety shall develop standardized intake questions that can be used by all Texas law-enforcement agencies to better identify whether a person calling the agency has information that should be reported to the Texas Suspicious Activity Reporting Network.
Within thirty days of this order, the Department of Public Safety shall develop clear guidance, based on the appropriate legal standard, for when and how Texas law-enforcement agencies should submit Suspicious Activity Reports.”‘
The question should be whether the “standardized questions” and reporting processes might have made a difference. Unfortunately, I’m not reading questions: I’m reading accusations that the Governor wants to impose “red flag laws” and confiscation of guns without due process of law.
The Governor previously directed the Texas Department of Public Safety to implement the “iWatch app” in June, 2018, allowing the public to report suspicious activity. There was no outcry then, and there doesn’t appear to be any “red flag” incidents because of this initiative.
Why do people think the Governor wants gun control now?
Children born overseas (No change)
The “Highlights:”
•Clarifies that temporary visits to the United States do not establish U.S. residence and explains the distinction between residence and physical presence in the United States.
• Explains that USCIS no longer considers children of U.S. government employees and U.S. armed forces members residing outside the United States as “residing in the United States” for purposes of acquiring citizenship under INA 320.3
Not the hype you’re reading about in the news.
Edit: Penultimate sentence: “18” instead of “28.” On September 3, 2019. BBN
Texas’ reaction
At least 22 people are dead and another 20 to 40 wounded in El Paso, Texas, due to a planned, murderous rampageby a man who drove 650+ miles to reach the site. He carried a semi-automatic rifle and wore both eye and ear protection.
The killings alone are enough to prove the killers are evil and full of hate, but their history and social media portray individuals focused on hate, erasing all doubt. It appears that the Texas shooter identified with white supremacists white supremacists while also professing to be anti-government and anti-corporation, while concerned about the environment. The Ohio shooter was known to be obsessed with guns, had participated while armed in a counter-protest against white supremacists and was politically left-leaning. The motives of the California shooter aren’t clear at all.
“””The age to purchase a firearm is 21. The state requires gun owners to obtain licenses and face background checks as well as imposing waiting periods on firearms purchases. Judges can take guns away from owners who are deemed to be a threat to themselves or others. And recent legislation aims to begin a fingerprinting database of all gun owners in the state.””
“””Apparently it doesn’t work like that. (Someone should tell our elected leaders.)””
Evil will find a way.
What will Texas response be?
In Texas, the result will probably be more guns.
Arguing Abortion on YouTube
I usually agree with this doctor. But not about abortion. ZDoggMD, Zubin Damania, has a sense of humor and a sense of balance. But today, he demands that we to “come to the center” because 1 in 4 women in the US have an abortion by age 45. “It happens.”
Well, according to the 1860 US Census, approximately 25% of families owned slaves. “It happen(ed).” Common ground was hard to find there, too.
The question is whether or not abortion ends the life of a human that is human-enough to possess the Human Right not to be killed. Are they one of us and can we kill them if they don’t threaten our lives?
The first question has been definitively answered, at least scientifically. Louise Brown was born 5 years after Roe v Wade. Serial ultrasounds showing the progression of the egg to embryonic organism to fetus were possible soon after. (I’m tempted to echo the ZDogg, “Grow up and get into the 21st Century.” But of course, I won’t.)
Answering these questions according to ethics and law can’t be addressed by science and requires a bit more discussion. Nevertheless, the trend in Western societies has been toward including all humans as rights bearers endowed with at least the right not to be killed or treated as the property of another and preventing legally sanctioned killing and enslavement, regardless of characteristics, abilities, or background.
Beyond the life of the mother, the rest of ZDogg’s arguments are the usual justification for what I call, “I want” ethics, including arguments for the “control of the woman’s body,” the health of the woman, and exceptions for rape and incest.
Nik Hoot, a 20 year old young man from Indiana, lost his feet and part of his legs and fingers to an attempted abortion, but survived to be adopted, eventually a State Semi Finals high school wrestler, and a productive member of society. His mother’s body didn’t lose limbs; his did. As he says, he has to “live with someone else’s choice.”
As to the health of the mother, how could anyone know at 12 weeks that there will be sequelae at or after delivery?
The safety of abortion is most often reported using short term data. There’s support for increased mortality and morbidity in the long term, however.
Late discovery of fetal abnormalities isn’t a good argument in favor of induced abortion, either. After 15 weeks and definitely after 20, it’s statically safer for the mother to carry to term.
I won’t even entertain arguments that crime is down because the unwanted are killed. “Minority Report” has a double meaning, here.
Let’s face it: the wrong human is killed by abortion justified by reason of rape or incest. If you cringe at that statement, you might want to consider why.
Beverly B Nuckols, MD
Updated information on TRTL, end of life, and money
One Texas Right to Life (TRTL) lawyer has posted an update on Facebook about the “rescue” of Mrs Carolyn Jones. I’m afraid that, as with the declaration that another patient was “slain,” TRTL is gaming the Medicare funding and Texas medical systems for political purposes.
Emily Cook, General Council for TRTL, wrote that she worried that “funny business clinically would happen as we moved her” from the hospital where Mrs. Jones has been admitted for over 6 months, where the docs had weaned her off the ventilator and wanted her to transfer to a more appropriate level of care facility over 2 months ago.
Emily says TRTL spent their own money (*see my last paragraph) to put her in a private ambulance and take Mrs. Jones to another hospital ER. That hospital couldn’t provide dialysis, so they in turn transferred her via ambulance somewhere else, to yet another hospital until admission can be arranged at the nursing home.

Cook-ing the system
Mrs. Jones’ Medicare funding for the original hospitalization is bound to have run out some time ago. Normally, Medicare will allow 90 days per admission, with an extra 60 “reserve” days, once per person, per lifetime. The patient is responsible for part of the bill from the first day of admission, and for the total hospital costs after the eligible days.
But there are still Medicare regulations to deal with in the case of “Medicare eligible” patients, even when they aren’t paying.
Medicare makes it very difficult and risky for everyone to navigate the private pay process. When I had a question in my private medical office about whether Medicare would cover something, we had the patient sign an informed consent agreement and an acknowledgement that the patient might have to eventually pay if Medicare denied the service. Then we performed the service, filed the charge with Medicare, waited to be denied, and then tried to Bill the patient. I gave away a lot tetanus vaccines and removed a lot of moles and warts for free to avoid the risk of “fraud and abuse” from the likes of Janet Reno.
The same risk would have applied if the hospital had privately charged Mrs. Jones’ Dialysis.
I don’t believe the first new hospital is at risk for a charge of “dumping” if they documented a legitimate reason. However, both new hospitals will be able to charge the Jones copays and co-insurance. They may also find Medicare coverage limited because of the way Mrs. Jones left the original.
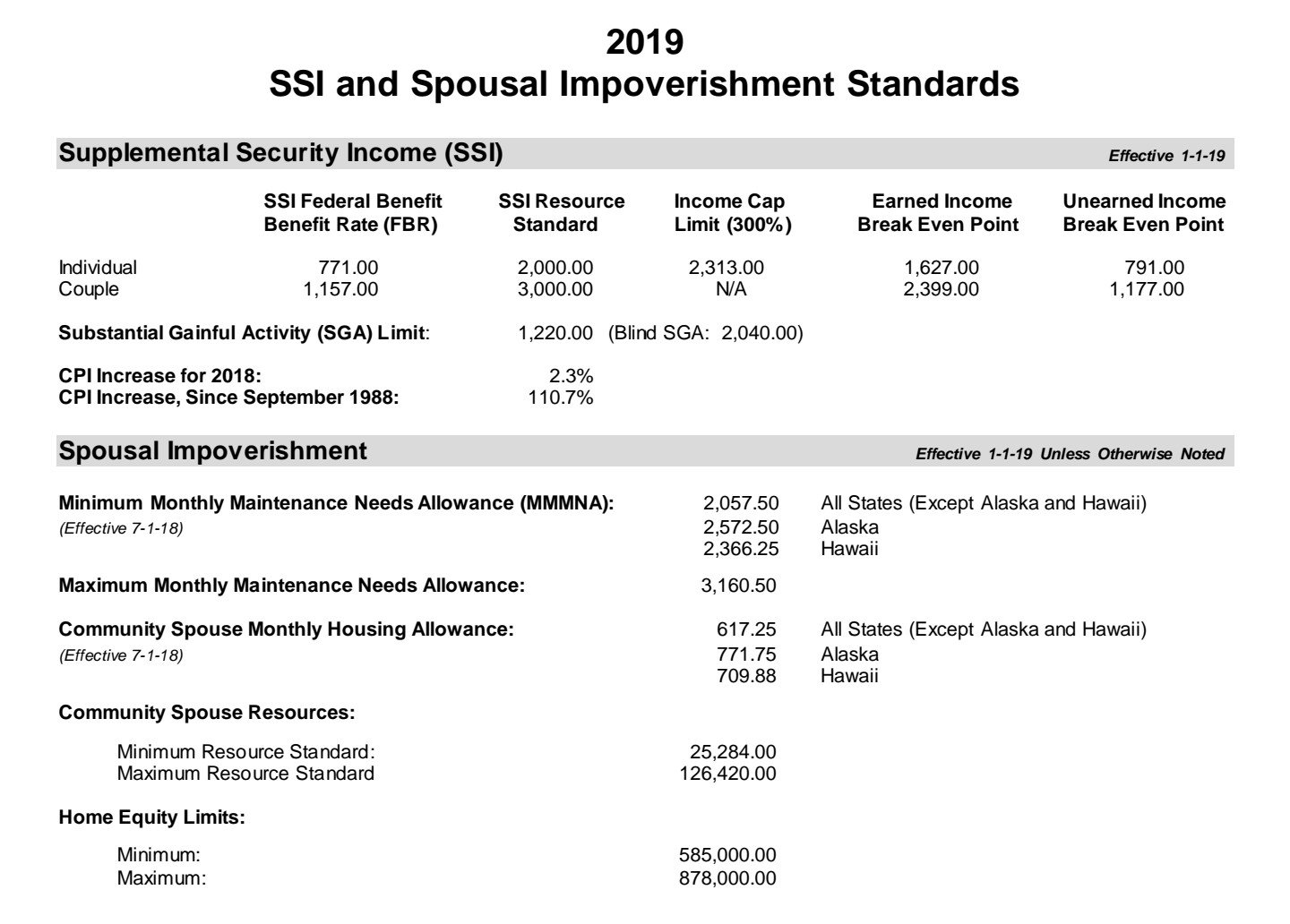
“Medicaid limits 2019” (a .PDF)
I certainly don’t know the Jones’ financial circumstances, and I may have over estimated the maximum income in early speculation. However, there are strict maximum Medicaid income and asset levels. These vary according to age, disability, and marital status. (Even the government bureaucratic Leviathan doesn’t want the spouse if a nursing home patient to end up indigent.)
In my experience, the social workers and benefits experts at hospitals and nursing homes are experts at negotiating and translating the bureaucracy. In addition, the disabled Medicare eligible person will have access to a benefits specialist. I’ve never had a hospital discharge and nursing home admission blocked by this “paperwork.” Certainly not for months at a time.
I hope TRTL assists the Jones family with what is certain to be several enormous hospital bills. As long as they pay the bills directly, the funds won’t be counted as income to Mrs. Jones.
End of life or end of hospital stay?

What a tragic story!
While I only know what I’ve seen online, in my experience, it appears that the dispute about Mrs. Carolyn Jones is over continued hospitalization at this hospital, versus transfer to care at another facility.
(See this television news report.)
I’m the first to say that hospitals are scary places and to sympathize with families struggling to cope with the bureaucracy and protocols. However the current news, press releases, and pro-life blogs are reporting several errors and omissions about Texas’s law and legislation up for consideration in Austin.
The obvious errors in this report include:
1. First. It’s not correct that Mrs Jones will die on Monday, even if the ventilator is turned off at the hospital. She’s not intubated through the mouth or nose. Instead, there’s a tracheostomy and a feeding tube in place. Supplemental oxygen could be provided many different ways, at home or in a nursing home.
2. Mr. Jones has testified at the Texas Senate Health and Human Services Committee meeting (EDIT: the video is here, at 52 minutes in) on 4/10/19 and elsewhere that Mrs Jones had been weaned off the ventilator, needing it only occasionally, at night.
2. She should be able to speak and swallow with training.
3. Texas Advance Directives Act doesn’t require that the doctor declare the treatment be “futile.” Instead, the doctor must declare that he refuses to follow a certain treatment decision that the patient or family demands .
4. Kidney dialysis is paid for by the Federal government, so the problem isn’t only funding.
In my admittedly limited knowledge about this particular case – it appears that Mr. Jones disagrees that it’s time to move from the hospital to home or nursing home, even after 5 months (not 10 days).
At least since 2005, legislation has been introduced at the State to increase the timeframe to as long as a month. Texas Right to Life refuses to agree to anything other than indefinite treatment, with the doctor forced to act against his will, violating his conscience and ignoring his medical judgement.
TRTL has even clashed with other pro-life organizations and Texas’s Catholic Bishops and “primaried” several conservative Legislators, although they are the only Texas pro-life group that opposes the law.
It would be good to add more time – I don’t know of anyone who disagrees. But there needs to be a limit to how long a doctor is forced to act against his conscience. One Bill that was rumored this year would change the “10 days” to 21 days and add a week to the notification period before the Ethics committee meets. Unfortunately, it never got past the Powers That Be.
For more on the ethics of the Texas Advance Directives Act, see this WingRight post.
The most urgent need is communication with families, correcting misunderstandings like those outlined here.
(Edited May 10, 2019 at 12:22 AST, to correct the Link to the testimony of Mr. Jones. BBN)
Emergency: Liberty Right Infringement
Texas Right to Life General Counsel Emily Cook is attacking Texas Medical Association on Facebook, even though virtually every other pro-life, medical, nursing, hospital, and disability group in Texas oppose SB 2089 by Hughes, that would change the “Texas Advance Directive Act, “TADA” will harm patients and attack the right of doctors to refuse to act against our conscience.
We’ve worked to fix other problems: Artificially administered food and water, even full IV feedings, can‘t be removed. Texas law didn’t even mention DNRs, but last session, we passed an amendment with explicit procedures and informed consent language.
There’s no leeway, at all, in the new Bill.
SB 2089 specifically says anyone can file a lawsuit in any Court in the County, the Court can’t charge the patient (or surrogates) any fees, and the judge is required to rule in 5 days.
If you believe that even doctors have the right of Conscience, and that infringement of the right not to be forced to act against your will is wrong, please contact your Texas Senator and Lieutenant Governor Dan Patrick and respectfully ask that SB2089 not be brought up.
You can let me know if you disagree on my Facebook page.
Another kind of lawyer joke
“[T]he doctor/bioethics committee thinks the patient should die.” Wesley J. Smith, Esq., Texas Senate Health and Human Services Committee, 4/10/2019 LifeNews.com
Wesley Smith is a rarity among the many lawyers who chased bioethics to the bedside late in the last century: he actually believes in the sanctity of human life and in the right of conscience. I’ve attended and reported on his debates and encounters with proponents of intentional euthanasia. And even happily defended him.
Unfortunately, Lawyer Smith was not above spinning the truth this month when he came from California to once again misrepresent the Texas Advance Directive Act (“TADA,” “the Act,” or “166.___”), an attempt to balance conflicting rights when doctors disagree with a patient or his surrogates about actual medical procedures and treatments that the doctor believes harms the patient.
On April 10, 2019 Mr. Smith gave invited testimony to the Senate Health and Human Services Committee in favor of SB 2089 (Hughes) and
SB 2129 (Creighton). LifeNews.com published part of his testimony online, under the title, “Texas Rule Allows Hospitals to Essentially Euthananize Patients After a 10-Day Notification.”
Mr. Smith doesn’t just contradict multiple Supreme Court rulings since Cruzan (1990) affirming that withholding or withdrawing treatment is not equivalent to euthanasia. Paradoxically, he echoes arguments that anti-conscience activists use to justify abortion on demand, Physician Assisted Suicide and intentional euthanasia by a third party by claiming that the principle of autonomy supercedes “First, do no harm,” or non-malevelence, and the right to conscience.
(You can watch all of Part I and Part II of the April 10, 2019 Health and Human Services Committee meeting addressing SB 2089 by Senator Bryan Hughes and SB 2129 by Senator Brandon Creighton online. Part I includes Mr. Smith’s testimony beginning at 33:00/1:01:10.)
We’ll skip Mr. Smith’s assertion that there is a right to force others to provide everyone medical care in general, not just in emergencies or at the end of life. I’ve covered these assertions and his attacks on the Texas Conference of Catholic Bishops I’m, back in 2007.
Today, let’s just look at his spin on the current version of TADA.
Lawyer Smith uses emotionally weighted terms that aren’t in TADA, such as, “life-extending,” “futile care,” “permitting the institution to force its will on patients and families,” “invidious discrimination,” and “inappropriate care.” He contrasts patient’s “rights” with doctor’s “values,” and is the first that day to raise the specter of doctors willing to kill when patients are “expensive.” And, reflected in the LifeNews.com headline, Mr. Smith flatly says that TADA allows euthanasia – intentional acts to kill patients – equivalent to the administration of injections or medications that he wrote about this week.
As I’ve stated so many times in past WingRight.org and LifeEthics.org posts, TADA doesn’t allow us to remove or withhold care for patients, only treatments that are “medically inappropriate.” There are no futile patients, only futile treatments that cause harm to the patient over and over, without any expectation of reversing organ failure after organ failure.
Mr. Smith also ignores the multiple attempts by the medical and pro-life community and Legislature to improve the law’s timeframe and communication, much as Senator Creighton’s Bill. One example from 2007, SB 439 by Senator Bob Deuell, would have required written notice and an offer of a private ethics consult to take place at least seven days before the hospital committee meeting. That Bill had a schedule for giving the patient or surrogates written information about the dispute process, copies of medical records, and lists of resources. The family would have been given access to the committee meeting, with their own advocates. When the committee agreed that the treatment requested was inappropriate, the family would have receive assistance in searching for7⅞ another doctor or facility for at least another 21 days. I believe that the Bill bogged down in the House because of opposition from Texas Right to Life to any Bill that did not include liability for doctors and the indefinite “treatment until transfer” in this year’s SB 2089.
In the last five minutes of the Part I video, another lawyer, Texas Right to Life General Council Emily Cook, gave us the best clue about the ultimate goal of her organization: “judicial review.”
Ms. Cook and Mr. Smith would have every one of these disputes settled by a Court. This is the Texas trial lawyers’ dream: a huge weapon against our State’s tort reform.
Today, the law specifically allows an appeal to a County probate judge when the Committee agrees with the doctor’s decision. SB 2129 allows a request for an injunction in any Court in the County, enabling “judge shopping.” Since it also prohibits the County from charging the patient or his surrogates any fees, the costs would fall solely on the County.
Ultimately, SB 2129 would make it much, much easier to sue the doctor and the hospital, moving Medical decision-making into the courtroom.
Most of the “stakeholders” for patient rights in Texas (including Texas Alliance for Life, Texas Baptist Christian Life Commission, Coalition of Texans With Disabilities, Texas Medical Association, Texas Hospital Association, Catholic Hospital Association, Texas Nurses Association, and the Texas Conference of Catholic Bishops and many others) oppose both of the Bills that Mr. Smith favored. Since SB 2129 would mandate that the County pick up any Court costs and that the judge make his ruling within five days, don’t be surprised if we hear objections from representatives of these parties, too.
So what’s the “joke?”
It could be the ridiculous notion that Lawyer Smith is a mind reader, able to discern the “invidious” motives for the “discrimination” he feels doctors and hospitals routinely practice:
“To fully comprehend the unjust nature of Texas law in this regard, realize that these “futile care” or “inappropriate care” decisions do not terminate treatment because it won’t work, but because it does. It is keeping the patient alive when the doctor/bioethics committee thinks the patient should die.” (Emphasis from LifeNews.com’s transcript.)
He repeatedly comments that physician’s decisions about medically appropriate treatment are subjective and that they (we) might “project their fears and their desires onto the patient” based on our “values,” rather than medical judgement based on repeated, at least once a day examination of the patient, reports by the nurses and staff and our education and experience.
The joke might be that Lawyer Smith volunteered that the indefinite, repeated evaluation and medical decision-making against the medical judgement of doctors would not be “slavery.” I would like to know what Lawyer Smith calls the legal requirement to use one’s body and brain to carry out actions, including writing orders for nurses and other medical staff, against your will.
It might be tragically funny to watch “judicial review” end up with the two sides hiring expert witnesses – doctors – to give the judge opposing views. There’s dark humor in the realization that ultimately the judge would order the original doctor to use her medical judgement to provide treatment – against her best medical judgement.
But the real joke is that “judicial review” risks the unintended consequence of decisions made by judges like the late t Judge George Greer, who Mr. Smith wrote about in this article.
Comments are closed. Please comment on my Facebook page.
Texas Advance Directive Act 2019 Legislature
“(22) in complying with the procedures outlined in Sections 166.045iand 166.046, Health and Safety Code, fails to make a reasonable effort to transfer a patient to a physician who is willing to comply with a directive.Amendment No. 5Representative Toth offered the following amendment to Amendment No. 4:Amend Amendment No.4 by Toth to CSHB 1504 on page 3, line 25, between “Code,” and “fails”, insert “willfully”.””
Prenatal manslaughter?
Something to consider, from a question on Facebook about abolishing abortion and my discussionof the human rights of prenatal human beings:
“I read the article. It seems filled with potholes to extend personhood to an embryo. Would then a mother who, through negligence, caused death or damage to the embryo, say [by] falling down the stairs or drinking alcohol, be guilty of manslaughter?“
My answer:
The prenatal human is undoubtedly a member of our species, correct?
The risk of abusive prosecuters doesn’t negate the human right not to be killed or justify two classes of human beings, some with human rights, some not human-enough. It certainly doesn’t justify the current abortion on demand: New York’s abortion until birth or Vermont’s proposedconstitutional amendment that prenatal humans “shall not have independent rights under law.”
This is where there is a clear physiologic and philosophic difference between negligence after birth and before. There is no other human relationship equivalent to pregnancy and gestation. Before birth, she’s harming herself first, the child secondarily.
Just as some people had to learn to accept the full humanity of emancipated slaves, there will be a learning curve for the full humanity of the prenatal human. We can do better than Reconstruction and much better than Jim Crow.
There’s previous experience taking the unique relationship into consideration. We already deal with children harmed by alcohol abuse or born addicted to illegal drugs every day.
While there have been abuses, like the drug testing of mothers in South Carolina, it has been more productive to treat addiction than to prosecute as crimes.
*********
Please comment at my Beverly Nuckols Facebook page.
Banned by prolife website
I’ve sat on this for 4 days, hoping for a response to the questions I sent to 2 of the ‘co-founders” and an editor of the website. (They only use those online forms, so I can’t follow up by email.)
So far, no response from any of the 3.
I’m not going to link to the website, but the address is in the photo.
Unfortunately, the division in the Texas prolife community is deep. The article I attempted to comment on quotes – and disputes – an article I wrote for Texas Alliance for Life a few years ago.
All I wanted to say was that I hope the readers will read that article.
Praying for peace.
(BTW, that case ruling came down in favor of Houston’s Methodist Hospital and the Texas First Court of Appeals refused to declare the Texas Advance Directive Act unconstitutional.)
Human rights =/= “Nature’s rights”
The “revolution” would be based on human rights, based on previous ethics discourse:
“For example, the 1776 American Declaration of Independence held that the rights to life, liberty, and the pursuit of happiness were self-evident. The 1789 French Declaration of the Rights of Man and of the Citizen announced that the purpose “of all political associations is the preservation of the natural and imprescriptible rights of man,” such as the right to liberty. These expressions of natural human rights provided a vocabulary for arguing that slavery and other rights violations were wrong. Following the devastating human rights violations of World War II, the United Nations adopted the Universal Declaration of Human Rights, recognizing the inherent dignity of all humans and a broad array of rights. Many of these rights are not yet a reality for many people, but the Declaration provides a moral blueprint for more-just societies.“Rights-of-nature advocates posit that environmental devastation is a moral wrong that ought to be stopped. This claim is not grounded in scientific evidence but is no less valid than the assertion that harming humans is a moral wrong. Neither human rights nor nature rights can be demonstrated through a scientific process, but we can make inferences about what justice requires on the basis of what we know to be necessary for the flourishing of humans or of nature.”
Guardians with appropriate expertise could be appointed as representatives.
And when the “guardians” see Nature’s rights as conflicting with our children’s, how well will that work out?
Educate and edify!
WingRight.org’s motto is the subject of today’s post. I hope to convince you of the necessity of speaking up in order to “educate” and “edify” (build up and strengthen) our neighbors and fellow citizens. ( We won’t get into the “elect” or pure politics.)
- Assume a pseudonym if you need to.
- Pick a subject or 2 that you feel comfortable “opining” about and act at least once a day.
- Pick just one website to influence, unless you have time to spread out.
- Ask advice from trusted sources when necessary.
- Be as accurate as you can be – at least, don’t lie or exaggerate for effect.
- You might come up with a stock statement that you copy and paste or modify where appropriate. Talking points are an effective tool.
- Ignore tacky responses and personal attacks – don’t be distracted or feel you are obligated to engage and argue if you don’t want to.
- Correct a mistatement, give a reference, or simply state your reasoned, opposing opinion.
Look at the bulk of comments out there, these tactics are the norm, not the exception.
(Comments are closed on the blog. You can respond on my Beverly Nuckols Facebook page.)
Bashing Trump: Victim shaming, victim denying
Toxic Fact checking!
Toronto Star Washington, DC reporter Daniel Dale (@ddale8) joins in the media’s Trump bashing, with some old fashioned victim shaming: foolish women are deceived into prostitution by “promises of a hopeful future,” not violently kidnapped, gagged and bound.
Well, not often enough for Mr. Dale.
Focusing on the type of tape that President Trump says was used to gag the women, Dale claims that he sought out “experts” who told him that physical, violent kidnapping of women in Mexico in order to traffic them – force them into prostitution – in the US “rarely if ever happens.”
Dale quotes a San Antonio “anti-trafficking activist” who woman who has helped 12 such women whose mouths were covered when they were kidnapped. Unfortunately, she didn’t record what was used to cover their mouths.
Oh, and the wall won’t change anything except that it “would merely cause certain traffickers to take more risks and impose higher debts.”
After all, less than 2% of women who are trafficked press kidnapping charges.
Dale might put too much weight in the fact that “less than 2%” of women who are trafficked press kidnapping charges. He should listen to the women of Jalisco who tell a story similar to the one the President relates. They then face the resistance of police and authorities with attitudes like Dale’s.
Just how many violent kidnappings across the border would be enough for Mr. Dale and his experts to report the stories of trafficked women instead of a story to prove President Trump wrong?
Cashless Society, Internet to Dystopia?
The dystopias of Rand’s Atlas Shrugged, Orwell’s 1984, or Bradbury’s Farenheit 451 had nothing available to monitor and police behavior and thought nearly as powerful as the Internet.
But that was *government* acting outside of Constitutional guidelines, not private business. . .
Facebook, Apple, Spotify, and YouTube ban and erase/delete Alex Jones on* the* same* day*? Only conspiracy nuts would see a conspiracy in the timing!
How do you feel about your credit card company conspiring and colluding with Internet platforms to monitor – and “de-monitize” – your actions and speech: “sins,” as arbitrarily determined by the arbitrary ethics or whims of a 3rd or 4th party?
Even if you don’t read Revelation as the prediction of the ultimate dystopia, you might agree that there’s a move to force political – ethical – correctness on the public by monitoring and restricting how you spend and receive money. You might even see the possibility that in order to spend and earn money, we could soon need the approval – the “Mark” if not of *the* “Beast, “of some lesser beast, composed of powerful organizations.
Real-World Consequences of Inappropriate Behavior
(Or, just like Europe today and the sometimes official reaction to raping immigrants.)
In a column in the National Review today, “The Real-World Consequences of Submitting to the Transgender Zeitgeist,” Ben Shapiro writes about a man who effectively ran off a group of religious, conservative women who cancelled their membership at a “women only” gym after a transgendered MtF (a man who claims to be a woman) began using the gym and dressing room.
The women had frequented the gym out of modesty: they didn’t want to see half-baked men or be seen by men in their workout clothes.
He refused the offer of a private dressing room (most women wouldn’t, I certainly wouldn’t!) and declared that since he is a woman he can undress with all the other women.
If he wants. That’s what it’s all about, right? His wants vs. age old cultural norms and thousands of years of religious modesty practice.
As time went on, he evidently continued to do the same. The gym manager was told by his bosses that the company couldn’t risk a lawsuit or boycott. So, the modest women left the gym and cancelled their memberships.
It’s not easy, and it would be vital to work together as a group. This isn’t a call for harassment. But, we each have the same right as this person to express our individual disapproval and to do it with our philisophical sisters, as others have done.
(And in reality, our brothers can’t act with the same righteousness as we can. A group of men objecting to a transgender woman in the same way would risk false harassment and assault charges.)
In a way, I’m writing this as my own protest. The social media Powers-That-Be are blocking people who object to the “new normal.”
Transgender First Principles

This weekend, the debate concerning the ethics of medical and surgical intervention for transgendered men and women, more properly called “gender dysphoria,” heated up again. The New York Times published an essay by a man who wishes to become a woman so much that he is about to undergo a 6 hour surgical procedure to fashion an artificial vagina, although the author admits that the surgery may not produce happiness and, indeed, will most certainly cause lifelong pain and the necessity of further intermittent, painful procedures.
In addition, one of the early leaders in the development of surgical procedures for trans persons, Dr. Phil McHugh, agrees that transgender ideation is a “Pathogenic meme.”
and schizophrenia, along with the “clusters” of peer-group rapid and late onset, as well as the rate of reversals, suggest caution when it comes to treatment that might later be considered disfiguring and permanent.
If doctors truly forget the First Principle, what’s to stop us from “First, doing harm?” Who decides the “harm” in that case? Better hope we don’t give up our consciences.
Please comment on my Facebook page, Beverly Nuckols.
American poor are middle class in world standards
I have so much to be thankful for this Thanksgiving Day. Unfortunately, there are people who think I should be ashamed instead.
So, in my geeky way, I did some research and found some information to have on hand the next time someone talks about the poor in the US.
Those poverty rates are based on income. SNAP, TANF, Section 8 vouchers,etc., aren’t counted as income. (You could add in our public education system, as well. If you believe it’s adequate.)
According to a report (in .pdf) by the Brookings Institute, using poverty measurements based on consumption or expenditures, those living under the poverty rate in the US would be considered middle class in the rest of the world.
“Even those reporting no income at all in the US have consumption possibilities roughly equal to those reporting incomes of $20 a day.”
Thankful for my wonderful husband, our shared faith in the Lord, our material blessings, and the Internet that enables my geekiness!
Click here to get your “Choose Life” license plate

Rick Perry RickPAC
Yes, I'm still for Governor Perry!
RickPAC
SiteMeter
