WingRight
Texas
Comprehensive review of Texas’ Heartbeat Act
Excellent, thorough, and true! Since I could never do better and can’t imagine editing, I’ve been given permission to copy & paste. Please give it your time and attention!
(The group is an excellent source & great to follow on Twitter, @secularprolife)
Secular Pro-Life Perspectives
Wednesday, September 29, 2021
The Texas Heartbeat Act: Answers to 11 Frequently-Asked Questions
Today’s guest post is by Daniel Gump.
After passage of the Texas Heartbeat Act (Senate Bill 8), numerous misinformation campaigns have led to confusion among the general public as to what the legislation covers and how violations are handled. Because of this, I have encountered several of the same questions and inaccurate statements repeated on social media over the past couple months. The following responses address some of these questions.
1. What is excluded from the definition of “abortion”?
Health and Safety Code already defines abortions under Sec. 245.002, and the Act did not amend them. Subsection (1) states:
(1) “Abortion” means the act of using or prescribing an instrument, a drug, a medicine, or any other substance, device, or means with the intent to cause the death of an unborn child of a woman known to be pregnant. The term does not include birth control devices or oral contraceptives. An act is not an abortion if the act is done with the intent to:
(A) save the life or preserve the health of an unborn child;
(B) remove a dead, unborn child whose death was caused by spontaneous abortion; or
(C) remove an ectopic pregnancy.
This definition is similar to those across the entire United States, as treatment for ectopic pregnancies and post-miscarriage treatment are not criminal acts in any jurisdiction. The laws solely address intentional acts of feticide.
2. How are medical emergencies handled?
The legislation declares for Health and Safety Code §171.203-§171.205 that abortions performed or induced for legitimate medical emergencies are exempted from prosecution. They must be logged in the woman’s medical records and retained in the physician’s own practice records.
The existing Sec. 171.002 defines what would be considered a medical emergency:
(3) “Medical emergency” means a life-threatening physical condition aggravated by, caused by, or arising from a pregnancy that, as certified by a physician, places the woman in danger of death or a serious risk of substantial impairment of a major bodily function unless an abortion is performed.
3. How are fetal anomalies addressed?
The Texas Heartbeat Act is silent on fetal anomalies of any type, so an unborn child with Down syndrome, spina bifida, hydrocephalus, or other conditions is protected from abortion, unless the pregnant woman’s life is in danger.
4. Could women be sued for procuring abortions in Texas?
No, Section 3 of the Act adds Sec. 171.206 to the Health and Safety Code. This includes the text:
(b) This subchapter may not be construed to:
(1) authorize the initiation of a cause of action against or the prosecution of a woman on whom an abortion is performed or induced or attempted to be performed or induced in violation of this subchapter;
(2) wholly or partly repeal, either expressly or by implication, any other statute that regulates or prohibits abortion, including Chapter 6-1/2, Title 71, Revised Statutes;
Several other statutes already protect women from criminal abortion liability. Examples within the same code Chapter 171 include:
Sec. 171.064. ADMINISTRATIVE PENALTY.
(b) A penalty may not be assessed under this section against a pregnant woman who receives a medical abortion.
Sec. 171.106. APPLICABILITY.
A woman on whom a partial-birth abortion is performed or attempted in violation of this subchapter may not be prosecuted under this subchapter or for conspiracy to commit a violation of this subchapter.
Sec. 171.152. DISMEMBERMENT ABORTIONS PROHIBITED.
(b) A woman on whom a dismemberment abortion is performed, an employee or agent acting under the direction of a physician who performs a dismemberment abortion, or a person who fills a prescription or provides equipment used in a dismemberment abortion does not violate Subsection (a).
Sec. 171.154. CONSTRUCTION OF SUBCHAPTER.
(d) This subchapter may not be construed to:
(1) authorize the prosecution of or a cause of action to be brought against a woman on whom an abortion is performed or induced in violation of this subchapter;
5. Could women be sued or held liable for leaving Texas to procure abortions in another state or country?
There would be no civil or criminal liabilities within Texas for women receiving abortions, so any such liabilities would fall under the jurisdictions where the abortions take place. Holding women liable for abortions is very rare in any nations following English common law (as the US does when no statutory law exists to the contrary).
Of all 50 states, the only ones that explicitly allow for women to be criminally liable for abortions are:
- Delaware (11 Del. Code §652) – Class A misdemeanor (past viability)
- Nevada (Nev. Rev. Stat. §200.220) – Manslaughter (past 24wk)
- Oklahoma (21 Okla. Stat. Cit. §652(E), §691(D), §713(C)) – Manslaughter (if during commission of another crime)
- Utah (Utah Code §76-5-201) – Women only exempted from homicide laws in regards to legal abortions or unintentional actions.
6. Could taxi drivers and rideshare drivers be liable for transporting women to receive abortions?
This would take a very liberal interpretation of the new Sec. 171.208(a) to include drivers under “any person who…”
- performs or induces an abortion in violation of this subchapter;
- knowingly engages in conduct that aids or abets the performance or inducement of an abortion, including paying for or reimbursing the costs of an abortion through insurance or otherwise, if the abortion is performed or induced in violation of this subchapter, regardless of whether the person knew or should have known that the abortion would be performed or induced in violation of this subchapter
- intends to engage in the conduct described by Subdivision (1) or (2).
Drivers are multiple degrees separated from (2) aiding or abetting “performance or inducement” of abortions, and they are not (3) intending such action by transporting customers between locations.
The claim that drivers would be liable was little more than a publicity stunt by Lyft to inject themselves into discussion on the legislation. In their press release, they were very careful to avoid use of the word “abortion” and repeatedly hid behind euphemisns like “healthcare they need,” “healthcare appointment,” “healthcare access,” etc. This made the Texas Heartbeat Act seem like its purpose was to block women from seeing their OB/GYNs or other healthcare practitioners.
Lyft also made it clear that drivers and riders should follow a don’t-ask-don’t-tell policy for any illegal activities. The press release closed out with an announcement of a legal defense fund for drivers ferrying women in violation of the Texas Heartbeat Act, a $1 million donation to Planned Parenthood, and a link (with tracking parameters in the URL) for individuals to further donate to Planned Parenthood.
7. Could the rapist of a woman receiving an abortion sue the physician or anyone else involved for $10,000?
No, Section 3 of the Act adds Sec. 171.208(j) to the Health and Safety Code that states:
Notwithstanding any other law, a civil action under this section may not be brought by a person who impregnated the abortion patient through an act of rape, sexual assault, incest, or any other act prohibited by Sections 22.011, 22.021, or 25.02, Penal Code.
The Penal Code sections referenced address “Sexual Assault,” “Aggravated Sexual Assault,” and “Prohibited Sexual Conduct,” respectively.
8. Can anyone claim “bounty” after an abortion is performed?
What makes the Texas Heartbeat Act unique among fetal heartbeat legislation is that it declares any non-government individual to have standing to sue. The claims of open bounty on abortion clinics are exaggerated, as generally only those close enough to the acts would have enough evidence to merit lawsuits. Presumably, those close enough would include the women who had the abortions, the father of the unborn children, any relatives or guardians of either, and possibly those within their inner circles.
A random individual would have difficulty presenting a strong case, particularly with HIPAA laws and Texas’ own privacy laws concerning abortion reporting under Chapter 171 of the Health and Safety Codes. Any individual performing or inducing abortions who provides enough details to the general public about specific violations would likely be in violation of several other laws, as well.
Any lawsuit would also have to follow established legal procedures in the state under the Civil Practice and Remedies Code, Code of Criminal Procedure, and any other applicable areas of the Revised Statutes. A state-wide free-for-all to claim $10,000 per violation is not likely, as a claimant would have to pay court fees and attorney fees on a lawsuit with dubious chance of actually succeeding. Plus, an award is only available once per violation (Sec. 171.208(c)).
On September 18, 2021, abortionist Alan Braid wrote an article for The Washington Post in which he admitted to violating the law. He was careful to avoid publicly disclosing specific details, but two individuals residing out of state (Oscar Stilley and Felipe N Gomez), nevertheless, filed lawsuits against him to test the law. As these cases are still pending, their merits are difficult to determine.
9. What method must be used to determine the fetal heartbeat?
Section 3 of the Act adds Sec. 171.203 to the Health and Safety Code, which describes the means as being “standard medical practice”:
(a) For the purposes of determining the presence of a fetal heartbeat under this section, “standard medical practice” includes employing the appropriate means of detecting the heartbeat based on the estimated gestational age of the unborn child and the condition of the woman and her pregnancy.
(b) Except as provided by Section 171.205, a physician may not knowingly perform or induce an abortion on a pregnant woman unless the physician has determined, in accordance with this section, whether the woman’s unborn child has a detectable fetal heartbeat.
(c) In making a determination under Subsection (b), the physician must use a test that is:
(1) consistent with the physician’s good faith and reasonable understanding of standard medical practice; and
(2) appropriate for the estimated gestational age of the unborn child and the condition of the pregnant woman and her pregnancy.
Any specific requirements for methods fall outside the scope of the legislation and within any medical licensing boards of medical associations.
10. How far into pregnancy does the abortion ban take effect?
Based upon the definitions in the new Health and Safety Code Sec. 171.201, there is no specific time period, as the ban is based upon the ability to detect a fetal heartbeat, using “standard medical practice.” From subsection 1:
“Fetal heartbeat” specifically means cardiac activity or the steady and repetitive rhythmic contraction of the fetal heart within the gestational sac.
Even though the term used is “fetal heartbeat,” the scope of the law includes embryos, based on subsection 7:
“Unborn child” means a human fetus or embryo in any stage of gestation from fertilization until birth.
The actual method of detecting the heartbeat of the embryo or fetus relies on the discretion of the one conducting the test.
Johns Hopkins Medicine states that a transvaginal ultrasound can detect the heartbeat by 5-6 weeks, and an abdominal ultrasound can detect one by 7-8 weeks. These are just estimates that can depend on a number of circumstances, like quality of equipment and training of the individual.
Sec. 171.203 requires a physician to record the method of detecting the fetal heartbeat and the estimated gestational age. Presumably, this would reduce purposeful attempts of deceit to circumvent the law.
11. Did the Texas legislature increase funding to social programs within the Texas Heartbeat Act?
Though not part of the same legislation, the state’s budget increased several social programs for the year.
The “Alternatives to Abortion” program under the Texas Health and Human Services has seen a budget increase every two years since its inception. For the 2022-2023 biennial budget earlier this year, there was a 25% increase from $80 million to $100 million. This program addresses financial and material needs of pregnant women and parents. The website lists examples of services:
- Counseling, mentoring, educational information and classes on pregnancy, parenting, adoption, life skills and employment readiness.
- Material assistance, such as car seats, clothing, diapers and formula.
- Care coordination through referrals to government assistance programs and other social services programs.
- Call center for information and appointment scheduling.
- Housing and support services through maternity homes.
Additionally, the budget increased the following:
- $135.5 million for various mental health programs
- $10.2 million for women’s health programs
- $123.5 million for rural hospitals
- $164.2 million relating to foster care
- $57.6 million for combatting human trafficking

Photo by Matt Walsh from Unsplash
Powered by Blogger.
Texas transgender (7 yo) case
I don’t believe it’s appropriate for a child to undergo transition at such an early age, but there’s a few gaps in this story.
There is very little media coverage of the case, with opinion from only one side published online. I picked the report about the court decision that’s most comprehensive, even with some errors.
Mostly, this appears to be an especially ugly divorce battle. The dispute about transition has been going on since the child was 3 years old.
The child is one of two twins conceived by in vitro fertilization using the father’s sperm and a donor egg. The mother carried the two to term and delivered.
The mother filed the suit to end joint custody, but the father demanded that the jury decide custody, rather than the judge.
The jury was charged with 2 questions: should one parent have sole custody and should that parent be Mr Younger. They answered yes and no: one should have sole custody, but it shouldn’t be the father. The judge will rule this week on who gets custody & conditions.
I’m not sure, but I’m reading that there’s no immediate plans for puberty blockers & finding quite a bit of info that the blockers aren’t permanent.
I can’t help but hope there’s more to this story, because I still can’t accept a decision like this, at this age.
Texas Governor Abbott on “Suspicious Activity”
Texas’ Governor Greg Abbott ( @GovAbbott ) isn’t trying to change Texas law with last week’s Executive Order – in contrast to the claims I’ve seen on my Facebook news feed.
Instead, he called for law enforcement agencies under the executive branch to establish policies and training, and financial incentives to encourage “improving reporting channels and closing ‘information gaps’ when members of the public or law enforcement agencies worry that a person might be a threat to commit violence.“
The last three mass shootings in Texas tell us that we need to improve how our law enforcement and agencies follow current law on following up on reports and investigations.
The Sutherland Springs Church shooter in South Texas should have been rejected at point of sale background check because of his prior conviction and incarceration for domestic violence crimes while in the military. Unfortunately, he was never reported to the Federal database. (And so, Texas law probably couldn’t have made any difference.)
However, the Odessa shooter threatened and brandished a weapon at his neighbor, but local Law Enforcement Officers didn’t follow up because his house wasn’t on their GPS maps and was difficult to find!
The El Paso shooter’s mother tried to report him, but the LEO who spoke to her on the phone dismissed her concerns. No record of the call was made, according to the Allen police department.
I’m not sure that current laws would have (or should have) allowed any action against the (future) shooter by authorities, but it looks like that question and reporting procedures are what Governor Abbott wants clarified. From the Executive Order:
“”Within thirty days of this order, the Texas Department of Public Safety shall develop standardized intake questions that can be used by all Texas law-enforcement agencies to better identify whether a person calling the agency has information that should be reported to the Texas Suspicious Activity Reporting Network.
Within thirty days of this order, the Department of Public Safety shall develop clear guidance, based on the appropriate legal standard, for when and how Texas law-enforcement agencies should submit Suspicious Activity Reports.”‘
The question should be whether the “standardized questions” and reporting processes might have made a difference. Unfortunately, I’m not reading questions: I’m reading accusations that the Governor wants to impose “red flag laws” and confiscation of guns without due process of law.
The Governor previously directed the Texas Department of Public Safety to implement the “iWatch app” in June, 2018, allowing the public to report suspicious activity. There was no outcry then, and there doesn’t appear to be any “red flag” incidents because of this initiative.
Why do people think the Governor wants gun control now?
Washington Post attacks Life via Texas
The Texas Medical Board this year reported that 25 Counties don’t have any physicians at all. Many Texas Counties are health care shortage areas because of there’s not enough population to keep doctors busy. And many high population centers are shortage areas because Texas has a doctor shortage over all.
In 2011, Texas cut virtually every item on our budget due to the requirement of the State Constitution to balance our budget. One measure used to balance the budget was to focus State healthcare dollars on County clinics and hospitals that provide comprehensive, continuing – not single organ system – care.
We could have done more if President Obama hadn’t blocked Texas from receiving Federal Women’s health or Family planning funds. Texas taxpayers paid into that Federal fund, but were denied its return to us. Texas did our best to fill in the gaps this lost funding created, allocating $32M of our State tax funds to Family Planning and Women’s Health programs in 2013-14.
In 2015, when the budget improved, we increased State spending for Women’s health and Family Planning beyond historic amounts. In 2019, nearly $400M was allocated, including raising the cut off for eligibility to 200% of the poverty level. $15M+ was set aside to improve post-partum care.
Nevermind that science affirms that the life of each human begins at fertilization. Or that “reproduction” has obviously occurred before any woman has an abortion, ending the life of that other body, her child. (Yes, one commenter tried to tell us that not only women seek abortions.)
But it’s the last paragraph that tells the truth about the author’s agenda, with a little side dressing of racism. Mr Rivard tells voters to end the ,”one-party state” – to force taxpayers to fund elective abortion for both citizens, non-citizens, and illegal aliens alike.
Edit 8/21/19 5:15 EST (France time) to fix typos. BBN
Texas’ reaction
At least 22 people are dead and another 20 to 40 wounded in El Paso, Texas, due to a planned, murderous rampageby a man who drove 650+ miles to reach the site. He carried a semi-automatic rifle and wore both eye and ear protection.
The killings alone are enough to prove the killers are evil and full of hate, but their history and social media portray individuals focused on hate, erasing all doubt. It appears that the Texas shooter identified with white supremacists white supremacists while also professing to be anti-government and anti-corporation, while concerned about the environment. The Ohio shooter was known to be obsessed with guns, had participated while armed in a counter-protest against white supremacists and was politically left-leaning. The motives of the California shooter aren’t clear at all.
“””The age to purchase a firearm is 21. The state requires gun owners to obtain licenses and face background checks as well as imposing waiting periods on firearms purchases. Judges can take guns away from owners who are deemed to be a threat to themselves or others. And recent legislation aims to begin a fingerprinting database of all gun owners in the state.””
“””Apparently it doesn’t work like that. (Someone should tell our elected leaders.)””
Evil will find a way.
What will Texas response be?
In Texas, the result will probably be more guns.
Updated information on TRTL, end of life, and money
One Texas Right to Life (TRTL) lawyer has posted an update on Facebook about the “rescue” of Mrs Carolyn Jones. I’m afraid that, as with the declaration that another patient was “slain,” TRTL is gaming the Medicare funding and Texas medical systems for political purposes.
Emily Cook, General Council for TRTL, wrote that she worried that “funny business clinically would happen as we moved her” from the hospital where Mrs. Jones has been admitted for over 6 months, where the docs had weaned her off the ventilator and wanted her to transfer to a more appropriate level of care facility over 2 months ago.
Emily says TRTL spent their own money (*see my last paragraph) to put her in a private ambulance and take Mrs. Jones to another hospital ER. That hospital couldn’t provide dialysis, so they in turn transferred her via ambulance somewhere else, to yet another hospital until admission can be arranged at the nursing home.

Cook-ing the system
Mrs. Jones’ Medicare funding for the original hospitalization is bound to have run out some time ago. Normally, Medicare will allow 90 days per admission, with an extra 60 “reserve” days, once per person, per lifetime. The patient is responsible for part of the bill from the first day of admission, and for the total hospital costs after the eligible days.
But there are still Medicare regulations to deal with in the case of “Medicare eligible” patients, even when they aren’t paying.
Medicare makes it very difficult and risky for everyone to navigate the private pay process. When I had a question in my private medical office about whether Medicare would cover something, we had the patient sign an informed consent agreement and an acknowledgement that the patient might have to eventually pay if Medicare denied the service. Then we performed the service, filed the charge with Medicare, waited to be denied, and then tried to Bill the patient. I gave away a lot tetanus vaccines and removed a lot of moles and warts for free to avoid the risk of “fraud and abuse” from the likes of Janet Reno.
The same risk would have applied if the hospital had privately charged Mrs. Jones’ Dialysis.
I don’t believe the first new hospital is at risk for a charge of “dumping” if they documented a legitimate reason. However, both new hospitals will be able to charge the Jones copays and co-insurance. They may also find Medicare coverage limited because of the way Mrs. Jones left the original.
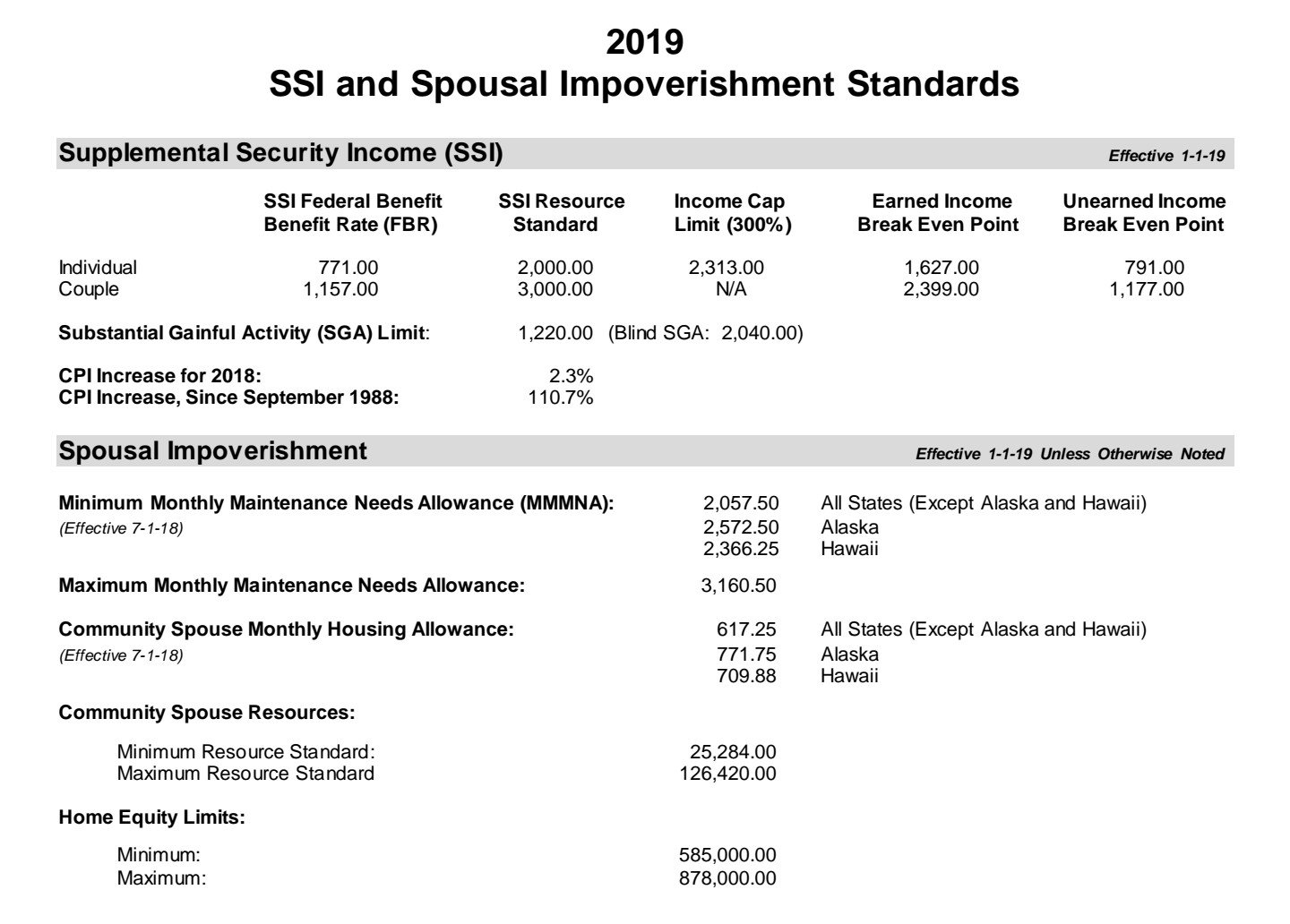
“Medicaid limits 2019” (a .PDF)
I certainly don’t know the Jones’ financial circumstances, and I may have over estimated the maximum income in early speculation. However, there are strict maximum Medicaid income and asset levels. These vary according to age, disability, and marital status. (Even the government bureaucratic Leviathan doesn’t want the spouse if a nursing home patient to end up indigent.)
In my experience, the social workers and benefits experts at hospitals and nursing homes are experts at negotiating and translating the bureaucracy. In addition, the disabled Medicare eligible person will have access to a benefits specialist. I’ve never had a hospital discharge and nursing home admission blocked by this “paperwork.” Certainly not for months at a time.
I hope TRTL assists the Jones family with what is certain to be several enormous hospital bills. As long as they pay the bills directly, the funds won’t be counted as income to Mrs. Jones.
Why does TRTL lie? (UPDATE)


they now post that a woman, Mrs. Carolyn Jones, had to be “rescued” from hers, “racing” to another facility “in the middle of the night.”
The family were given notice that they needed to transfer Mrs. Jones in March. They’ve had another doctor and three facilities capable of providing the treatments she needs waiting to accept Mrs. Jones.

And now, TRTL – in direct competition with – and with absolutely no mention of – Mrs. Jones’ family’s GoFundMe campaign – has been raising money in Mrs. Jones’ name. They state that the funds will be used for (TRTL) lawyer’s fees in addition to Mrs. Jones’ healthcare needs and that “excess” funds will go to help (TRTL’S) efforts for other patients.
I hope that TRTL’s money will also be used to pay for the very large hospital and doctor’s bills that the Jones family will receive. While there’s a chance that Texas Medicaid will pay for three months of medical bills, retroactively, Medicare doesn’t pay for hospitalizations over 90 days and has a 20% co-insurance (co-pay).
That’s bound to have added up in over 6 months.
We’ll just have to trust that TRTL won’t lie again.
Edit, Updated information:
One of the bloggers has told us more about that “rescue.” (Or today’s story, anyway.)
TRTL put her in a private ambulance and took her to *another ER,* one that couldn’t provide dialysis, so they then transferred her somewhere else.
There were comments about the first Hospital refusing transfer — no, refusing to be complicit with “dumping” a patient. Discharging to without ( or even with) acceptance of the transfer from the docs at the other facility is highly irregular and likely illegal.
Much has been said about funding. Yes. It appears that Medicare funding ran out, so no longer paying. 90 days per admission, with an extra 60 days over, under certain conditions.
About that Medicaid funding: I don’t know the limits of the mandatory asset tests, but the yearly income level is $60,000. One way to adapt is to spend money on medical costs.
Medicare makes it difficult to navigate the private pay process. When we had some question, we got informed consent, promise to pay, then performed the service, filed with Medicare, waited to be denied, then tried to Bill the patient. The risk is always a charge of “fraud and abuse.”
The same thing would have happened if the hospital had privately charged for Dialysis.
(5/20/19, BBN)
False story about Texas Advance Directives Act (TADA)
Mrs. Jones is not dependent on the ventilator.
In fact, it sounds like Mrs. Jones has had excellent treatment at the hospital,
Mr. Jones told the Texas Senate Health and Human Services Committee that the doctors at the hospital successfully weaned Mrs. Jones from the ventilator.
He also said that three other facilities are ready for her admission.
I’m happy to see that today’s article by reporter Tony Guajardo quotes both opponents and supporters of TADA and corrected the impression that Mrs Jones is dependent on the ventilator: “She requires dialysis, occasionally needs a ventilator for breathing assistance, and uses a feeding tube.“
And yet, today’s The Texan article still misrepresents this case: “UPDATE: Recovering Beaumont Woman’s Life-Sustaining Treatment to End Due to 10-Day Rule.”
There’s also a quote from Mrs. Jones’ daughter, repeated from the earlier article: ““My mom is going to die on Monday because of a law that saves hospitals money.”
It turns out that money and Medicaid paperwork is actually what is keeping the family from allowing Mrs. Jones to be transferred to another doctor and facility. The family is concerned that they (rather than the hospital) will be responsible for the costs of Mrs. Jones’ care.
This is in spite of the fact that when a patient first goes on dialysis, she becomes immediately and automatically eligible to apply for Medicare and Social Security Disability.
Depending on assets and income, patients unable to work on dialysis also qualify for Medicaid and other State benefits in Texas. Medicaid will even pay bills retroactively for three months.
The good news is that she isn’t dependent on the ventilator, dialysis is not constant but only 2-3 times per week and paid by Medicare, food and water by the feeding tube can’t be withheld under TADA.
Hopefully, the Jones family will finally agree to transfer her, even if costs them more than her Medicare & Social Security Disability will pay.
Have they no decency?
Now, Texas Right to Life is blatantly lying, posting an article on their website entitled “American hero slain two days before Christmas …”

“slain?”
Far down in the piece, there’s this:
“Chris passed away naturally on December 23, 2015 – two days before Christmas.”
Mr. Dunn died from his metastatic pancreas cancer, on full medical treatments. His mother, Mrs. Kelly actually thanked those who cared for him at the hospital.
Every article on TRTL’s website has a “Donate” button at the top, prioritizing money over the people whose stories they use to raise money and influence the Texas Legislature. Now, we see this completely dishonest caption.
Just what is their mission and how can we trust them?
Hurting patients and families
I don’t understand why TRTL repeats that a ventilator tube prevents Mrs. Jones from speaking or eating. Mrs. Jones has a tracheostomy in place (the tube we see in the pictures is a feeding tube). The tracheostomy, even when a ventilator is attached, would not interfere with her ability to speak and swallow, with training.
End of life or end of hospital stay?

What a tragic story!
While I only know what I’ve seen online, in my experience, it appears that the dispute about Mrs. Carolyn Jones is over continued hospitalization at this hospital, versus transfer to care at another facility.
(See this television news report.)
I’m the first to say that hospitals are scary places and to sympathize with families struggling to cope with the bureaucracy and protocols. However the current news, press releases, and pro-life blogs are reporting several errors and omissions about Texas’s law and legislation up for consideration in Austin.
The obvious errors in this report include:
1. First. It’s not correct that Mrs Jones will die on Monday, even if the ventilator is turned off at the hospital. She’s not intubated through the mouth or nose. Instead, there’s a tracheostomy and a feeding tube in place. Supplemental oxygen could be provided many different ways, at home or in a nursing home.
2. Mr. Jones has testified at the Texas Senate Health and Human Services Committee meeting (EDIT: the video is here, at 52 minutes in) on 4/10/19 and elsewhere that Mrs Jones had been weaned off the ventilator, needing it only occasionally, at night.
2. She should be able to speak and swallow with training.
3. Texas Advance Directives Act doesn’t require that the doctor declare the treatment be “futile.” Instead, the doctor must declare that he refuses to follow a certain treatment decision that the patient or family demands .
4. Kidney dialysis is paid for by the Federal government, so the problem isn’t only funding.
In my admittedly limited knowledge about this particular case – it appears that Mr. Jones disagrees that it’s time to move from the hospital to home or nursing home, even after 5 months (not 10 days).
At least since 2005, legislation has been introduced at the State to increase the timeframe to as long as a month. Texas Right to Life refuses to agree to anything other than indefinite treatment, with the doctor forced to act against his will, violating his conscience and ignoring his medical judgement.
TRTL has even clashed with other pro-life organizations and Texas’s Catholic Bishops and “primaried” several conservative Legislators, although they are the only Texas pro-life group that opposes the law.
It would be good to add more time – I don’t know of anyone who disagrees. But there needs to be a limit to how long a doctor is forced to act against his conscience. One Bill that was rumored this year would change the “10 days” to 21 days and add a week to the notification period before the Ethics committee meets. Unfortunately, it never got past the Powers That Be.
For more on the ethics of the Texas Advance Directives Act, see this WingRight post.
The most urgent need is communication with families, correcting misunderstandings like those outlined here.
(Edited May 10, 2019 at 12:22 AST, to correct the Link to the testimony of Mr. Jones. BBN)
Another kind of lawyer joke
“[T]he doctor/bioethics committee thinks the patient should die.” Wesley J. Smith, Esq., Texas Senate Health and Human Services Committee, 4/10/2019 LifeNews.com
Wesley Smith is a rarity among the many lawyers who chased bioethics to the bedside late in the last century: he actually believes in the sanctity of human life and in the right of conscience. I’ve attended and reported on his debates and encounters with proponents of intentional euthanasia. And even happily defended him.
Unfortunately, Lawyer Smith was not above spinning the truth this month when he came from California to once again misrepresent the Texas Advance Directive Act (“TADA,” “the Act,” or “166.___”), an attempt to balance conflicting rights when doctors disagree with a patient or his surrogates about actual medical procedures and treatments that the doctor believes harms the patient.
On April 10, 2019 Mr. Smith gave invited testimony to the Senate Health and Human Services Committee in favor of SB 2089 (Hughes) and
SB 2129 (Creighton). LifeNews.com published part of his testimony online, under the title, “Texas Rule Allows Hospitals to Essentially Euthananize Patients After a 10-Day Notification.”
Mr. Smith doesn’t just contradict multiple Supreme Court rulings since Cruzan (1990) affirming that withholding or withdrawing treatment is not equivalent to euthanasia. Paradoxically, he echoes arguments that anti-conscience activists use to justify abortion on demand, Physician Assisted Suicide and intentional euthanasia by a third party by claiming that the principle of autonomy supercedes “First, do no harm,” or non-malevelence, and the right to conscience.
(You can watch all of Part I and Part II of the April 10, 2019 Health and Human Services Committee meeting addressing SB 2089 by Senator Bryan Hughes and SB 2129 by Senator Brandon Creighton online. Part I includes Mr. Smith’s testimony beginning at 33:00/1:01:10.)
We’ll skip Mr. Smith’s assertion that there is a right to force others to provide everyone medical care in general, not just in emergencies or at the end of life. I’ve covered these assertions and his attacks on the Texas Conference of Catholic Bishops I’m, back in 2007.
Today, let’s just look at his spin on the current version of TADA.
Lawyer Smith uses emotionally weighted terms that aren’t in TADA, such as, “life-extending,” “futile care,” “permitting the institution to force its will on patients and families,” “invidious discrimination,” and “inappropriate care.” He contrasts patient’s “rights” with doctor’s “values,” and is the first that day to raise the specter of doctors willing to kill when patients are “expensive.” And, reflected in the LifeNews.com headline, Mr. Smith flatly says that TADA allows euthanasia – intentional acts to kill patients – equivalent to the administration of injections or medications that he wrote about this week.
As I’ve stated so many times in past WingRight.org and LifeEthics.org posts, TADA doesn’t allow us to remove or withhold care for patients, only treatments that are “medically inappropriate.” There are no futile patients, only futile treatments that cause harm to the patient over and over, without any expectation of reversing organ failure after organ failure.
Mr. Smith also ignores the multiple attempts by the medical and pro-life community and Legislature to improve the law’s timeframe and communication, much as Senator Creighton’s Bill. One example from 2007, SB 439 by Senator Bob Deuell, would have required written notice and an offer of a private ethics consult to take place at least seven days before the hospital committee meeting. That Bill had a schedule for giving the patient or surrogates written information about the dispute process, copies of medical records, and lists of resources. The family would have been given access to the committee meeting, with their own advocates. When the committee agreed that the treatment requested was inappropriate, the family would have receive assistance in searching for7⅞ another doctor or facility for at least another 21 days. I believe that the Bill bogged down in the House because of opposition from Texas Right to Life to any Bill that did not include liability for doctors and the indefinite “treatment until transfer” in this year’s SB 2089.
In the last five minutes of the Part I video, another lawyer, Texas Right to Life General Council Emily Cook, gave us the best clue about the ultimate goal of her organization: “judicial review.”
Ms. Cook and Mr. Smith would have every one of these disputes settled by a Court. This is the Texas trial lawyers’ dream: a huge weapon against our State’s tort reform.
Today, the law specifically allows an appeal to a County probate judge when the Committee agrees with the doctor’s decision. SB 2129 allows a request for an injunction in any Court in the County, enabling “judge shopping.” Since it also prohibits the County from charging the patient or his surrogates any fees, the costs would fall solely on the County.
Ultimately, SB 2129 would make it much, much easier to sue the doctor and the hospital, moving Medical decision-making into the courtroom.
Most of the “stakeholders” for patient rights in Texas (including Texas Alliance for Life, Texas Baptist Christian Life Commission, Coalition of Texans With Disabilities, Texas Medical Association, Texas Hospital Association, Catholic Hospital Association, Texas Nurses Association, and the Texas Conference of Catholic Bishops and many others) oppose both of the Bills that Mr. Smith favored. Since SB 2129 would mandate that the County pick up any Court costs and that the judge make his ruling within five days, don’t be surprised if we hear objections from representatives of these parties, too.
So what’s the “joke?”
It could be the ridiculous notion that Lawyer Smith is a mind reader, able to discern the “invidious” motives for the “discrimination” he feels doctors and hospitals routinely practice:
“To fully comprehend the unjust nature of Texas law in this regard, realize that these “futile care” or “inappropriate care” decisions do not terminate treatment because it won’t work, but because it does. It is keeping the patient alive when the doctor/bioethics committee thinks the patient should die.” (Emphasis from LifeNews.com’s transcript.)
He repeatedly comments that physician’s decisions about medically appropriate treatment are subjective and that they (we) might “project their fears and their desires onto the patient” based on our “values,” rather than medical judgement based on repeated, at least once a day examination of the patient, reports by the nurses and staff and our education and experience.
The joke might be that Lawyer Smith volunteered that the indefinite, repeated evaluation and medical decision-making against the medical judgement of doctors would not be “slavery.” I would like to know what Lawyer Smith calls the legal requirement to use one’s body and brain to carry out actions, including writing orders for nurses and other medical staff, against your will.
It might be tragically funny to watch “judicial review” end up with the two sides hiring expert witnesses – doctors – to give the judge opposing views. There’s dark humor in the realization that ultimately the judge would order the original doctor to use her medical judgement to provide treatment – against her best medical judgement.
But the real joke is that “judicial review” risks the unintended consequence of decisions made by judges like the late t Judge George Greer, who Mr. Smith wrote about in this article.
Comments are closed. Please comment on my Facebook page.
Don’t mess with Texas Republican Women!
Mama had surgery for Thymic carcinoma back in 2004. She voted early and scheduled the surgery for the day after the election, so her daughters could work as election clerks.
Health care poll

Today, I came across a poll of likely Texas voters, conducted by the University of Texas and Texas Tribune that said that for Texans, health care is a distant third in importance, behind border security and immigration. This was in contrast with frequent news reports in the last week that an unnamed “recent poll” had found that health care is the number one issue in the 2018 election for voters. That first, UT/TT, poll was more consistent with other recent news coverage and the issues that I keep seeing pop up on Twitter and Facebook.
So I did some research….
It turns out that the first poll (“KFF,” download pdf file,with results) was conducted by the Kaiser Family Foundation, a nonprofit based in San Francisco, California. In fact, approximately 30% of the respondents listed health care as their number one issue and were designated “Health Care Voters” by pollsters. 70%, designated “non-Health Care Voters,” chose other issues, including the economy and jobs (21%).

The demographics of those polled were heavily slanted toward Democrats, with registered Democrats and “Independents” who are identified as “Independent Lean Democrat” adding up to 68% of the “Healthcare Voters.” “Non-Health Care Voters” came in at 49% Republican or “Independent Leans Republican.”
While KFF is considered one of the “Least Biased” polling bodies, they are still subject to sampling errors. It appears that this might be one of those times.
Comments are disabled. Comment on my Facebook page, please.
Sanctuary City Swimming in Other People’s Taxes
From the Mayor of the home town of La Joya Independent School District, the “independent” school system in Hildalgo County, Texas with the water park, a 22K sq ft natatorium, tennis courts, a planetarium, and a golf course,enabled with money from Texas taxpayers:
“My position was why should the city of La Joya, or any city in the Valley, detain any ICE illegals when ICE already has cages for them?”Salinas said Sunday. “Maybe they have a better place for them than we do and, of course, we’re totally against what they’re doing; I think we should unite the families, not divide them.”
…
“If it hadn’t been for that I would not have reacted this way,” he said, “but I’m a Mexican-American and I support my people.”
It’s not just “that.”

people.
Edited to correct spelling. BBN
Happy Birth Parent Day

- Google Images for “Baby Daddy” card
That lawsuit I wrote about yesterday would not only would put an end to Texas’ Medical and legal regulations on abortion – including informed consent, waiting periods, and sonograms – the plaintiffs go out of their way to redefine mother and father, too.
“”1 Most people with the capacity to become pregnant identify as women. Historically, both jurisprudence and public health data have focused on women when addressing reproductive rights and health. But there is an emerging recognition in the law and society more generally that not all people who may become pregnant identify as women. See generally Glenn v. Brumby, 663 F.3d 1312, 1316-19 (11th Cir. 2011)(holding, consistent with the weight of authority, that the Equal Protection Clause prohibits discrimination on the basis of “gender nonconformity”) (collecting cases); Robin Marantz Henig, How Science Is Helping Us Understand Gender, National Geographic (2017), https://www.nationalgeographic.com/magazine/2017/01/how-science-helps-us-understand-gender-identity/. The Constitution protects the rightof all individuals to end an unwanted pregnancy, regardless of gender identity.”
From the UK, we see the inevitable results in a time of identity and personal choice :
“Lawyers have told a judge that he had been biologically able to become pregnant but had legally become a man when the child was born.
“They say the transgender man wants to be identified as the child’s “father” or “parent” on a birth certificate.”
And, in Ohio:
“Explaining their unusual parenting arrangements, Amy said: “We went through a lot of fertility treatments, until we finally reached a point where we needed to make a decision as to whether we were going to do more medical intervention or if we were going to switch bodies. (emphasis mine)
“We were fortunate enough to have two uteruses. So, after a lot of thought and emotion and difficulties we switched to Chris.
“And while Chris lived as a man and didn’t feel female, he was willing to use his womb for the good of their family.”
Of course, neither Chris nor Amy could donate sperm. So, who is really — is there even — a father?
Or a parent, of either gender or any identity, who sees the child as his own person, human-enough to possess inalienable rights, rather than a political statement and a means to an end?
Open letter to RPT Convention delegates on censure
I am writing to ask you to vote against censure by the Convention of named Republican, elected, officials.
How often have we complained about the elites who get in power only to ignore us to follow their own agenda? How many of you are at the Convention because you got tired of the establishment working against you?
Well, guess what? If you make it to the State Convention, you’re the elite establishment! Don’t be that kind of elite establishment.
For the first time in years, I couldn’t participate in the 2018 Republican Party of Texas Convention process. I still follow your efforts and have read the resolutions submitted to the Platform Committee. One Senate District has submitted resolutions demanding that the RPT State Convention censure specific legislators.
I appreciate the work you’re doing this not just this week, but over the last few months. Having served as a Delegate to the Republican Party of Texas State Convention and on both the Platform and the Rules Committees, I know you have a week of long walks to simply get to your meeting rooms, heated discussions, long waits, and many re-votes, one after another. The Committees and sessions start early and go late. (Wear comfortable shoes and take snacks!)
Through all of this, please don’t forget that you are in San Antonio as the grass roots embodiment of our Nation’s representative democracy, our Republic. You are not simply individuals expressing your own will and opinion. You are there as representatives of your constituents: the Republican voters from your Counties, Congressional Districts, and Senate Districts.
In the same way that you expect legislators to represent their voters, your voters expect you to represent us.
While it may be appropriate for the local SD Convention to censure their own legislators, especially before the Primary or run-off, many people in our Party disagree. But now, these are elected candidates. I don’t believe that it’s appropriate for the State Convention to censure them in opposition to the local electorate’s wishes.
When the votes on censure of any Republican elected official comes up, please take a look at their constituents’ votes, especially in the last Primary. Did he or she win? Was it by a substantial margin? Was he or she unopposed in the Primary because no one even challenged them?
These men and women deserve your respect, just as President Donald Trump should be given the respect he deserves after being elected President. In the same way that it was wrong for Hillary to deride Republican women as voting the way their husbands told them to, it’s wrong to dismiss these voters as illegitimate.
In addition, as this is an election year, you are writing the campaign ads for the Democrats.
Please do not oppose the voters you represent by voting in favor of public censure of Republicans.
Beverly B. Nuckols, MD
Comal County, SD 25 and CD 21
(Edited because some of the formatting got lost.)
Response to criticism about Texas Advance Directive Act
I’ve been having a long Facebook discussion with representatives of organizations, people who claim that I support coercion and killing patients because I defend the Texas Advance Directives Act, 166.0046. (TADA).
I want to respond as fully as I can. ( I’m bandwidth deprived today and will gradually add more links when I reach better signals. See here, here, and here for more explanations from earlier WingRight posts. Links to the law, the press, and previous blog posts by others can be found in those articles.)
It was easy to follow this case. There was a video published by Texas Right to Life (TRTL), a lot of press, statements to reporters by family, lawyers, and TRTL staffers, as well as a couple of lawsuits. I spent the better part of two days once again reviewing the public records.
It
(Edited 03/11/18 for typos, to add a link, and to clarify points originally made on Facebook in a long debate. BBN)
Latest story on ethical stem cells in Texas
Last week, in a story about another baby boy, there was a a beautiful memorial to the “Bubble Boy,” David Vetter, too.
The story in the Houston Chronicle is also a tribute to the doctors and parents who keep immune compromised children alive while waiting for the cure or treatment to take effect.
My granddaughter’s mother is one of those heroes, helped by doctors and nurses, my son and an extended family of friends. (I can’t help my prejudice that gives the mother most of the credit.) And then, there was a baby boy and his generous mother.
I told Roni’s story to the Texas Legislature back in 2007 and 2006. An anonymous baby boy and his parents saved Roni’s life in 2001.
In addition to a very low white blood cells count, her bone marrow didn’t make enough red blood cells or platelets, either. She’s healthy and well, today, after one of the first cord blood bone marrow transplants in the world at the age of 15 months.
Although no matches were found for Sebastian, the baby in today’s story, Texas has a strong system for the registration of both bone marrow and umbilical cord blood donors. The Texas Cord Blood and MD Anderson Cord Blood Centers collect, store s and manage the distribution of donated cord blood collected at birth from moms and babies all over the State.
Families who store their baby’s cord blood privately are very unlikely to ever need it, except when there’s a known problem. The odds are less than 1:200,000. But if they donate to a public bank, the blood is much more likely to save a life and/or be used in life-saving research.
Bravo to all the parents and caregivers in children’s lives and prayers for Sebastian. There’s a Go-Fund-Me account for Sebastian’s expenses, if you are interested.
Edit: there’s a wonderful update: Sebastian was able to go home!
“Different” (Transgender at 4?)
The TexasGOPVote website chronicles the complaint by a “Conservative, Christian” mom that her male to female (supposedly) transgender 6 year old shouldn’t be treated differently. I agree with the underlying sentiment that it is not the child’s fault.
The child is treated differently – by parents, peers, school nurses, and any educator, doctor or other professional or official who is complicit with this abuse of a 6 year old child – because the child *is* different. Medicine, physics, and the rest of the observable, measurable and verifiable universe don’t change because a child declares that cold is hot, up is down or boys don’t feel like “she” feels (at the highly experienced age of 6).
It is disturbing to read about the apparent mistreatment of depression that this mother describes in her earlier blog. So disturbing that I’m inclined to ignore – or at least put off to another post – commenting on the stereotype in the description of “girly girl, Kai, in pink and sparkles” or of the suggestion in mom’s earlier blog about Joseph as “gay” (at 2!) for displaying supposedly “flamboyantly feminine mannerisms and love for all things girly.”
How could anyone so misinterpret the repeatedly voiced desire of a 4 year old to be taken away to heaven because another 4 year old said her father called him a freak as equivalent to hating hair cuts ( or more “feminine mannerisms“)? How can she compare her “secret” research with the proper treatment her son needed?
Unfortunately, a 6 year old claiming to be transgender is different because he or she has had his or her perceptions of the world colored by the same adults who would not allow a child they loved to play with fire or jump off the highest point of the school building.
The fact is that genetic and phenotypically female girls will always be “different” from Joseph. From the first penetration of the zona pellucida by a sperm bearing a Y chromosome, to the differentiation of the Wolffian duct, to the first time he urinated over someone’s shoulder into the air after birth, Joseph has been a male. Stereotypes aside, he will remain a male, however he acts or is medically or surgically manipulated. The genetic and phenotypical reality of his body will always affect any future medical or surgical treatment.
Hopefully, no one will be complicit with medical or surgical castration or other mutilation until this child is legally competent to consent. In that case, his body will still be phenotypically male, entering puberty, when he enters middle school, whether as as Joseph or Kai. Now, that will be a “difference” evident to all the girls, including the ones who have never seen male genitals.
It will be very evident to the survivors of sexual abuse. Hopefully, they called the police after they were abused.
Contrary to the claim in the blog, Lt. Governor Patrick and the “Bathroom Bill” didn’t start the trans debate. School districts in Texas were changing policies, entire cities have passed ordinances, and the last President issued an Executive Order that threatened Federal education dollars.
And preditors are taking advantage of the increased access available due to the transgender debate: men like Paul Witherspoon, Levandus Gacutan, Christopher Hambrook, Richard Rodriquez, Jason Pomare, Sean Patrick Smith, or the many unnamed men who have been not reported to the police when they enter previously gender-segregated areas like poolside changing rooms, shower rooms or gym locker rooms. (I’ll let you research those names.)
Thanks to “Conservative, Christian” mom, the world is being misrepresented to other children who are encouraged to consider pathological behavior as not “different.” Because of “feelings” the rest of us are repeatedly told to ignore the difference – and observable, measurable, and verifiable facts.
And this specific child is being abused.
Beverly B Nuckols, MD.
Equal, but special
A Facebook friend, Michael Smith, made an excellent comment about the contrast between “separate but equal,” and “equal, but special.”
I spent some time yesterday at the Texas State Capitol Reagan Building discussing House Bill 2899 by Simmons, which would prohibit local governments and other regulatory authorities from creating a new “order, ordinance, or other measure to protect a class of persons from discrimination; to reduce or expand a class of persons protected under state law from discrimination.”
The consensus of a group of people waiting for the House State Affairs Committee to begin was that the Bill is a thinly veiled “attack” on the LGBT community and transgender persons in particular. The comment that made me go into my Don Quixote tilting windmills mode was about just wanting to “peeing in peace” and the false claims of fears for safety of women and children.
I pointed out that that it is reasonable for women to have fear when confronting a man in a closed space and that we all expected privacy and security in bathrooms, locker rooms and other public places where people disrobe. (Yes, I used the term “disrobe.” And “intimate spaces.” I’m a nerd.)
I was told that I was speaking from “privilege” (!) for my example of caution when entering an elevator with a strange man and objecting to the stereotype that the brains of men and women are different and the assertion that men and women simply think differently. I heard that segregation of the sexes in public bathrooms is a new phenomenon and that the Roman baths, such as those in Pompeii were completely different matters, mainly due to the religion of the time. And of course, several of the group told of the danger of violence against gays or trans but that there has never been any crime against other people by transgender person
Two of the people claimed to be transitioned from male to female. While demanding “respect,” they told stories of having coworkers fired for refusing to use their preferred pronouns. and engaged in very real “hate speech,” mocking and assigning hateful motives and emotions to me. The same person who pointed out that little boys can be molested in men’s bathrooms then said that *I* was the one who must obviously consider anyone with a penis a predator.
The group was secure in the belief that the fears of violence and abuse of the LGBT community outweigh not only the fears of victims of sexual abuse or parents of children and thousands of years of social norms.
Cities, but claiming to write non-discrimination ordinances create environments where some people are “equal, but special” – or a specially protected class of persons. George Orwell put it another way: “Some animals are more equal than others.”
Law makers to doctors: “Keep the patient alive”
If only we doctors – or legislators, lawyers and probate judges – really had the power to “keep the patient alive” as this article claims two new Bills ( HB 4090 & SB 1213) in front of the Texas Legislature will (force doctors to) do.
The article is misleading in its claim that a committee or a hospital decides whether or not a therapy is given: Texas doctors practice medicine in Texas. Even the Bills make it clear that the “attending physician” makes the decision whether or not to follow the patient’s (or more likely, the surrogates’) medical request.
We – Texas doctors, hospitals, and legislators – have tried repeatedly over the last decade to amend the law, Texas’ Advance Directive Act, to increase the time frame. Last Session, we helped to ensure that food and water can’t be withheld. The lawyers and those who would have Estate (probate) judges involved in every dispute – even at the bedside of the dying – have blocked effort after effort because the Bills did not include liability for the doctor.
These Bills are just the camel’s nose under the tent of Texas’s tort reform. Worse yet, we’d end up with medical expert testifying against medical expert in court, with the judge eventually telling the doctor how to practice medicine. It would also severe the “ethicists” who actively seek to undermine conscience protections for health care professionals.
If you’ll notice, the Bills also remove the requirement for the patient to pay for any transfer, too. I don’t suppose that the tort lawyers will pay for the ambulance or plane ride.
Do you want Texas law to force doctors to practice against our consciences?
How long and how far should any man or woman be forced by law to act against his or her will?
Texas “Bathroom Bill”

(Photo of the men’s bathhouse at Pompeii, in contradiction to the claim that gender-segregated facilities are a modern concept.)
The Texas Senate State Affairs has another long day ahead, as testimony will be heard today on SB6, the so-called “Bathroom Bill.”
Here’s a rebuttal that I wrote in response to a facetious op-ed that appeared in the Austin American Statesman last month. The Opinion editor told me a shorter version would be published, but I haven’t seen it.
Obviously, John Kelso isn’t a survivor of male on female sexual abuse or harassment.
Many survivors (like me, at 3 years old) have strong reactions to the idea – the threat – of a man in the enclosed space of even a “public” bathroom. Just as as I worry about the safety of children, I also want a “safe space,” where I am not likely to be confronted by a male.
If the transgendered individual doesn’t trigger that fear – and I have no doubt that I’ve shared bathrooms with some who didn’t – then no problem. However, their ability to do so is no justification to engage in sweeping social experiments.
Representative Schaefer and Lieutenant Governor Patrick didn’t start this controversy. Individuals making policy decisions in cities, school districts and the Federal government did, sometimes with the weight, fines, and penalties of law.
The fact is that at least 1 in 5 women have been sexually abused before the age of 18. (In my experience as a Family Physician, I would have expected the percentages to be higher.) More than 90% of those assaults are committed by males who prey on females. While “only” 20% or so are perpetrated by strangers, isn’t that enough?
And yes, some of us do consider innocence a value to be protected and wish to protect girls from involuntary exposure to the physical characteristics of anatomical males. Thus, our objection to co-ed bathrooms and the Obama Administration’s Department of Education guide lines that included locker rooms and overnight accommodations on school trips.
Significantly, Kelso claims to be ignorant of multiple abuses of by straight males, dressed as females or otherwise, who take advantage of the opportunity to exploit newly accessible, formerly same-sex, hygiene facilities. I suggest at least a bit of online research.
How dare commenters mock women’s “worry” and “FEAR(sic)?” Isn’t fear of assault the reason most often given to justify “gender neutral” policies?
Would you like to refuse?
Shocking Bill from Texas’ Jason Villaba, Republican State Representative from Dallas’ District 114 : HB 1938 would make organ donation after death “opt out” for anyone applying for a driver’s license in Texas.
Texas would be the first State to pass such a law.
Organ donation is a public good for those who wish to do so. However, there is no ethical or legal precedent for treating human bodies – living or dead – as public property or commodities.
From the Bill as introduced:
(2) for an applicant who is 18 years of age or older: (A) specifically ask each applicant the question, “Would you like to refuse to join the organ donor registry?” and state, “If you answer ‘no’ to the previous question or do not answer the previous question, you consent to join the organ donor registry by performing either of those actions.”; and (B) if the applicant does not affirmatively refuse to be included in the registry under Paragraph (A), provide the person’s name, date of birth, driver’s license number, most recent address, and other information needed for identification purposes at the time of donation to the nonprofit organization contracted to maintain the statewide donor registry under Section 692A.020, Health and Safety Code, for inclusion in the registry.
http://www.legis.state.tx.us/tlodocs/85R/billtext/html/HB01938I.htm
Trump can’t run 3rd Party in Texas?
Read the Texas Secretary of State information page on Presidential candidates, here. (http://www.sos.state.tx.us/elections/candidates/guide/president.shtml )
I’m not a lawyer, but it appears to me that Texas election laws will prevent Trump from placing his name on the ballot as a 3rd Party candidate in 2016.
Any lawyers disagree?
Texas’ Republican Platform 2016
 About 300 delegates to the RPT weren’t Republican.The Platform of the Republican Party of Texas is online under “Platform,” here: http://www.texasgop.org/2016-convention/ . The numbering in this version of the Platform is awkward, but the plank-by-plank votes are reported at the 3rd link, below.
About 300 delegates to the RPT weren’t Republican.The Platform of the Republican Party of Texas is online under “Platform,” here: http://www.texasgop.org/2016-convention/ . The numbering in this version of the Platform is awkward, but the plank-by-plank votes are reported at the 3rd link, below.
110 even voted against Principle #5, “Personal accountability and responsibility”
Just under 300 voted consistently against what should be non-controversial issues, such as the plank against human trafficking.
(Numbering appears to be a typographical error, hopefully soon corrected. The hard copies we had were much clearer.)
https://www.texasgop.org/wp-content/uploads/2016/01/PERMENANT-PLATFORM-as-Amended-by-Gen-Body-5.13.16.pdf
https://www.texasgop.org/wp-content/uploads/2016/01/2016-Texas-GOP-Weighted-Totals-.pdf
Counting win before chicks are hatched.

If Ted Cruz wins Presidency, it leaves a huge blank if Cruz resigns before Obama is out.
A special election will be called for the next uniform election day or 32 days after election is called.
We’ll need Cruz to resign as soon as elected or wait until inauguration to prevent aggression by the “Office of the Lame Duck President.”
Posted from WordPress for Android. Typos will be corrected!
I’m quoted in Houston Chronicle about Supreme Court hearing
By 7 PM, there was a line of people setting up to spend the night in front of the Supreme Court of the United States building. They hope to be able to watch the Court proceedings on Wednesday when the Texas abortion law, HB2.
Here’s the coverage from Brian Rosenthal of the Houston Chronicle, about Texans, like me, who travelled to DC for the hearing. I’m quoted as ‘helpful about the future of the law in the last few paragraphs.
Beverly Nuckols, 60, a New Braunfels family doctor who flew in for the arguments, said she was happy that a long and just process finally could be coming to an end.
Nuckols said was hopeful about the ruling because she was confident in the law.
“I believe we will get a tie,” she said.
Texas Governor Greg Abbott endorses Cruz for President
Huge endorsement from Texas’ Governor Greg Abbott. This is one I had been wondering about.
In a video announcing the endorsement, Abbott said,
“Unlike far too many in Washington, the Ted Cruz we’ve seen in the Senate is the same Ted Cruz we elected and he’s the same Ted Cruz I served with when I was attorney general,” Abbott said.
I was very impressed and very proud of Ted Cruz back in 2009, on the day when Kay Bailey Hutchison announced that she would run one more time as Texas’ Senator. Within minutes, Cruz withdrew his bid for Attorney General, rather than run against General Abbott. Although later I became opposed to his campaign tactics, that moment showed integrity.
( I’m just barely cynical enough to think it also showed good political sense. In fact, that only just occurred to me. Doggone it! I want to believe it was character, not simply savvy politics.)
Cruz needs mentoring – to *accept mentoring* – from both Governor Perry, who has also endorsed Cruz, and from Governor Abbott. I hope that he will.
Death Politics
Someone named Rich DeOtte has written a Facebook piece attacking friends of mine. Rich mocks Dr. Joe Pojman as “a rocket scientist” and “knucklehead” (needless to say, that’s not popular in the Nuckols household) and takes a slap at Kyleen Wright, of Texans for Life Coalition and the Texas Medical Association.
Dr. Joe Pojman, Ph.D., is indeed a “rocket scientist,” who gave up his original career path of aerospace engineering to sacrifice as founder and Executive Director of Texas Alliance for Life, an organization I’m proud to support and serve as a Board member.
Joe wrote the op-ed that Rich attacks in direct response to the “misrepresentations” in another, political op-ed piece by Emily Kebedeaux Cook on the Texas Right to Life Website. Joe only wrote about issues, and did not engage in name calling or derision. The only reason Emily and TRTL are mentioned is because she’s the author of the political opinion piece about the “decline in the Texas Legislature’s efforts to protect human Life.”
As Joe points out, the very document to which Emily refers refutes her position: Texas was named one of three “Life List All-Stars” for 2016 by the Americans United for Life.
Joe laid out the case that our Texas Legislature’s pro-life laws are most definitely not at a standstill: we are ahead of the Nation. Joe’s position that Texas leaders gave us many successes in the 2015 84th Legislature is supported by the similar list of “Wins” reported by the Texas Catholic Conference, representing the Bishops of Texas. In an earlier letter, TCC notes that many of the criticisms Emily makes in her February 8th blog post were not previously scored “equitably” by TRTL. For instance, Senator Bob Deuell received no credit for authoring much of what became HB2.
In fact, Texas’ Legislative leadership in passing pro-life laws is why many of us are going to Washington, DC on March 2nd to bear witness when the Supreme Court hears testimony on the abortion facility regulations in HB2.
Emily and Rich focus most of their criticism on the efforts of pro-life groups, including doctors like me, to reform end of life care and the Texas Advance Directive Act (TADA). Session after session since it was passed, we in the pro-life community have had our efforts repeatedly blocked by the “death panel” accusations Rich makes and the demands in Emily’s op-ed.
I was one of the doctors appointed to the Texas Medical Association ad hoc committee that evaluated last sessions’ end of life Bills for TMA approval. Our group of doctors agreed to and helped fine tune HB 3074, what Emily called a “modest protection”: prohibiting the removal of Artificially Administered Nutrition and Hydration, including food and water by invasive medical methods like IV’s and “Total Parenteral Nutrition.” We were called anti-life and pro-“death panel” (Rich’s words) for including medical exceptions for the rare circumstances when the patient can’t process the AANH and/or when it actually caused harm.
Those “three strongest Pro-Life bills” that Emily mentioned were included in the “Wins” listed by the TCC. The Bills not only would have forced doctors to continue to indefinitely perform acts that we believe are not medically appropriate as long as a patient or his family demands it. They would have forced all disputes between the doctors practicing medicine and patients or their families into court and add “liability”(civil and criminal penalties) for the doctor.
Forget if you can, that if all disputes go to court judges would be required to determine medical care – to practice medicine – probably based on the testimony of dueling, paid medical expert doctors. Malpractice rates will go up for doctors taking on the most vulnerable patients – the elderly, the trauma victims and the victims of cancer. Those doctors will spend more time in courts, rather than in the ICU. And so will more grieving families.
We found out what happens when malpractice goes up in Texas, before tort reform was passed. Because of the malpractice crisis, there were no neurosurgeons west and south of San Antonio and Houston – none at all in El Paso or all of South Texas. We were losing obstetricians and family doctors willing to deliver babies and offer prenatal care, all over the State.
I don’t know how to translate past physician shortages directly into the possible shortage of doctors providing end of life care. However, I will predict that fewer family doctors, internists, pulmonologists and the ICU intensivists will be able to afford to practice in the ICU. Just as a patient had to be flown to Dallas, San Antonio or Houston from most of Texas for a head injury, only the tertiary medical centers in those cities will be able to staff their ICU’s properly.
Physicians, not hospitals – and certainly not courts – practice medicine in Texas. Doctors must be allowed to practice medicine according to our medical judgment, which is a combination of education and experience, under the watchful eye of the community; not “death panels,” but fellow physicians, nurses, ethicists, lawyers (who may be any of the former) and lay people. In the end, if you force the hands and minds of doctors against their judgment, you will end up with doctors practicing without judgment, and humans with inalienable rights forced to act against our will and in violation of our conscience.
And, now, back to Rich’s Facebook post. Think twice when you read political posts full of personal attacks and name calling. We should be able to discuss politics without, as Emily said in her blog post, “unnecessary, vicious, and vindictive fights inside the Republican Party.”
Edited to fix a name glitch – BBN
Click here to get your “Choose Life” license plate

Rick Perry RickPAC
Yes, I'm still for Governor Perry!
RickPAC
SiteMeter
