WingRight
Technology
Long Post Reviewing COVID19 Myths
I’m often asked to comment on medical issues by friends. I’ve been having a Messaging conversation with a libertarian friend about what I consider myths. Here’s a loooong post, based on that conversation. I’m not linking to his reference videos, but you can search for them (or ask on my Facebook page) if you really want to give them the “clicks.” Comments should also be made on Facebook. (Keeping comments more public as well as trying to avoid “blog-pimping.”)
The problem I’ve seen is mixing criticism about policy (politics) errors from the actual science. It’s important to separate the science myths from the evidence for science facts. This “ZDoggMD” (Zubin Damania, MD) video is a good place to start for an overview. https://youtu.be/v8RpPeXCySw
As is this one, between Dr. Damania and Dr. Mike (Mikhail Varshavski, DO) who, in another useful (and easy to watch) conversation,
https://youtu.be/XVjLT3pinW0
point out that it’s not wrong to be skeptical and question data. While reviewing the science and the scientific method, they discuss the harm from tribalism and politicization. Also, at 59 minutes, there’s an explanation about how the variants arise.
However, the skeptics are wrong to dismiss all data from formal regulatory and research sources. The scientific literature is best evaluated over time and in proportion with the number of supporting reports. As in the case of the Wuhan doctors who stood against their government to call the world’s attention to the outbreak in the first place, minority reports should be considered. The valid reports will stand the test of time, public scrutiny, and real world observation. In contrast, as in the case of the (infamous) retracted papers in Lancet and JAMA, questionable data will be disproven.
If we can’t agree on the above paragraph, there’s no common ground for discussion.
As for the questions I often receive about my personal sources (in reality, my integrity): I use as many sites as possible. I certainly do not refer to only one silo of information. And, yes, I have watched all of the videos people share – at least until last night, when my friend linked to ten. I have worked through over half of them, and watched the first part of all of those.
I prefer to evaluate the myths themselves, rarely discussing the validity of the sources, except to point out those falsehoods or to point out obvious pre-existing biases based on the statements of the speakers themselves.
For instance, there are repeated referrals to Robert F Kennedy, Jr., who isn’t a good source. He has made inaccurate claims about vaccines for years, shifting from blaming measles vaccines to aluminum and mercury & he makes money from his anti-vaccine advocacy.
The doctor at the school board meeting loses validity right from the first by flatly stating that masks cannot protect from any virus. Surgical masks and N95s work. https://www.aerzteblatt.de/int/archive/article/217467
He repeatedly talks about “the vaccine,” when there are at least four, developed by different companies, tested in different sites. Are all the nurses and other personnel involved going along with some conspiracy(ies) promulgated by corrupt doctors and companies?
He is absolutely mistaken about enhancement by the vaccines – as Dr. Zubin Damania pointed out in the first video above, real world observation on the sheer numbers of vaccinated disprove this myth.
The event he referenced about in Barnstable, Massachusetts is an anomaly, due to large indoor gatherings.
https://www.cdc.gov/mmwr/volumes/70/wr/mm7031e2.htm
The pdf of the actual report is here https://www.cdc.gov/mmwr/volumes/70/wr/pdfs/mm7031e2-H.pdf
In fact, Barnstable answers the doctor’s question about why we’re seeing a surge in summer: people who were previously “socially distanced” are now gathering with fewer precautions. (Add the fact that the biggest breakouts are occurring in areas where close spaces and air conditioning are predominant.)
In the rest of the world, the vaccinated are less likely to get infected at all. At least 1/3 less likely, perhaps closer to 90%.
(This is pre-peer-reviewed data.)
https://spiral.imperial.ac.uk/handle/10044/1/90800
https://www.medrxiv.org/content/10.1101/2021.06.28.21259420v2?ijkey=43686632fd3918a950438cfefd8a2fc06e73b0ac&keytype2=tf_ipsecsha
In one video recommended, Geert Vanden Bossche, DMV, PhD, who is a frequently referred to, emphatically states that there is a virus, that it is highly infectious and it is deadly and that the vaccines are “excellent” & prevent disease – meaning the severe effects of infection. However, since they do prevent infection, I believe he is wrong about using vaccines in the middle of the pandemic.
The largest number of people becoming infected, and by corollary, becoming infectious, symptomatic, requiring hospitalization and dying, are unvaccinated. What we are seeing is that the vaccinated who do get infected are less sick – even though they are older and have more comorbidities.
There may be a kernel of truth in what Bossche says (in spite of the decreased numbers infected), since the vaccines were authorized first for the elderly and sick, who were also most likely to have an incomplete immune response.
Vanden Bossche proposes that the variants come from patients with partial immunity in the same way that antibiotic resistance occurs when bacteria are exposed to antibiotics in already infected patients. As pointed out in the Dr Z and Dr. Mike explanation about how viruses mutate, the variants occur after thousands or millions of replications in infected people. The viruses first have to infect, then they have to survive and be infectious.
The vaccinated are much less likely to get infected in the first place so the numbers of infections that are necessary to happen for the event of mutations and spread to others occur in the unvaccinated. So fewer infections mean less chances to mutate.
Vanden Bossche doesn’t answer the question: “What do we do?” The alternative was to let them get sick and risk death, a risk which is much greater in this population than in younger people who likely have a stronger immune response.
Mike Yeadon, Ph.D. is another “expert ” that is frequently referenced because he once was a head researcher and CEO at Pfizer. He was one members of the team that did early mRNA vaccine research. Even he notes that he repeats that government shouldn’t be trusted. Included in contradictory statements, he claims that there’s no virus, after saying older and sicker people should probably choose to be vaccinated. What infection is Bossche talking about if Yeadon is right?
There’s an emotional video at the “A Warrior” vlog that has too many distractions to be useful in fighting for sane policy, with its emphasis on 9-11 and pedophile truthers. But I’ll cover some of the obvious errors:
Dr Sam Smith is wrong about the SARS-1 animal experiments. https://www.google.com/amp/s/mobile.reuters.com/article/amp/idUSKBN2A22UW
Il repeat: Do you believe that any group is powerful enough to suppress the observation of the effects of 500,000,000 doses of different vaccines all over the world – 350 million in the US, alone? – by the hundreds of thousands of doctors & even more nurses and other professionals who are involved and would need to be complicit?
Smith’s major objection is the regulation of treatments and what he believes is a politically motivated exaggerated risk of COVID. However, I know several people who have been hospitalized with the infection, and several friends have lost relatively young loved ones to it. I’m sure you have the same experience.
An August 26, 2021 “McCullough Report” podcast begins with a major myth: that there are 90% false positives in asymptomatic testing. That number might actually be 2-3% for saliva tests. But is closer to 1%. Confirmatory tests are recommended for any positive test.
https://pubmed.ncbi.nlm.nih.gov/34238663/
https://pubmed.ncbi.nlm.nih.gov/34223865/
https://pubmed.ncbi.nlm.nih.gov/34116245/
(McCullough does quote the correct percentage of hospitalized cases which are vaccinated in the UK and Israel: 40%. This number should be evaluated in relation to the percentageof vaccinatedin the community and who is getting sick. Both countries have a majority of elderly, who are likely to have less immunity efficacy, and were the first eligible for vaccination roll outs. These are also the people who are getting sick.)
BTW, going to integrity and trust, Zubin Damania has been active for years in fighting the politicization and socialization of medicine in the US, as have I. Google his conversations with Dr. Atlas, and two of the authors of the Great Barrington Declaration (which I also signed), Dr. Jay Bhattacharya and Dr. Sunetra Gupta. We are all secure in supporting vaccination, opposed to blanket lockdowns, draconian enforcement, and politicization of treatments by physicians.
Healing Spinal Cord Injuries By Reprogramming Cells | Worldhealth.net Anti-Aging News
“[W]e may not need to transplant cells from the outside.”
Good news from Texas medical researchers!
It appears that specific stimulating factors may prove more useful in harnessing the body’s own ability to heal and regenerate than stem cells, whether from my the patient or someone else. This research into regeneration of nerve cells mirrors the use of epogen and nupogen long used to induce blood cell production.
https://www.worldhealth.net/news/healing-spinal-cord-injuries-reprogramming-cells
EDITED TO ADD:
Here’s a longer online article from “EurekaAlert!,” from the American Assocation for the Advancement of Science, publishers of the journal, Science.
A modest proposal for COVID-19 response (Or, I’m not King, but)

JAMA table 1, comparing efficacy of masks
If I were in charge of the public health response to COVID-19, I would implement the following:
Pharmacy Boards should never get between a doctor and patient except in matters of life and death or illegal practice. Politicians, State Medical Boards and our House of Medicine professional organizations should defend our legal practice of medicine rather than threatening physicians and changing the rules during a pandemic.
2. Encourage shared information & fact-checking among physicians as part of our missions of education & transparency.
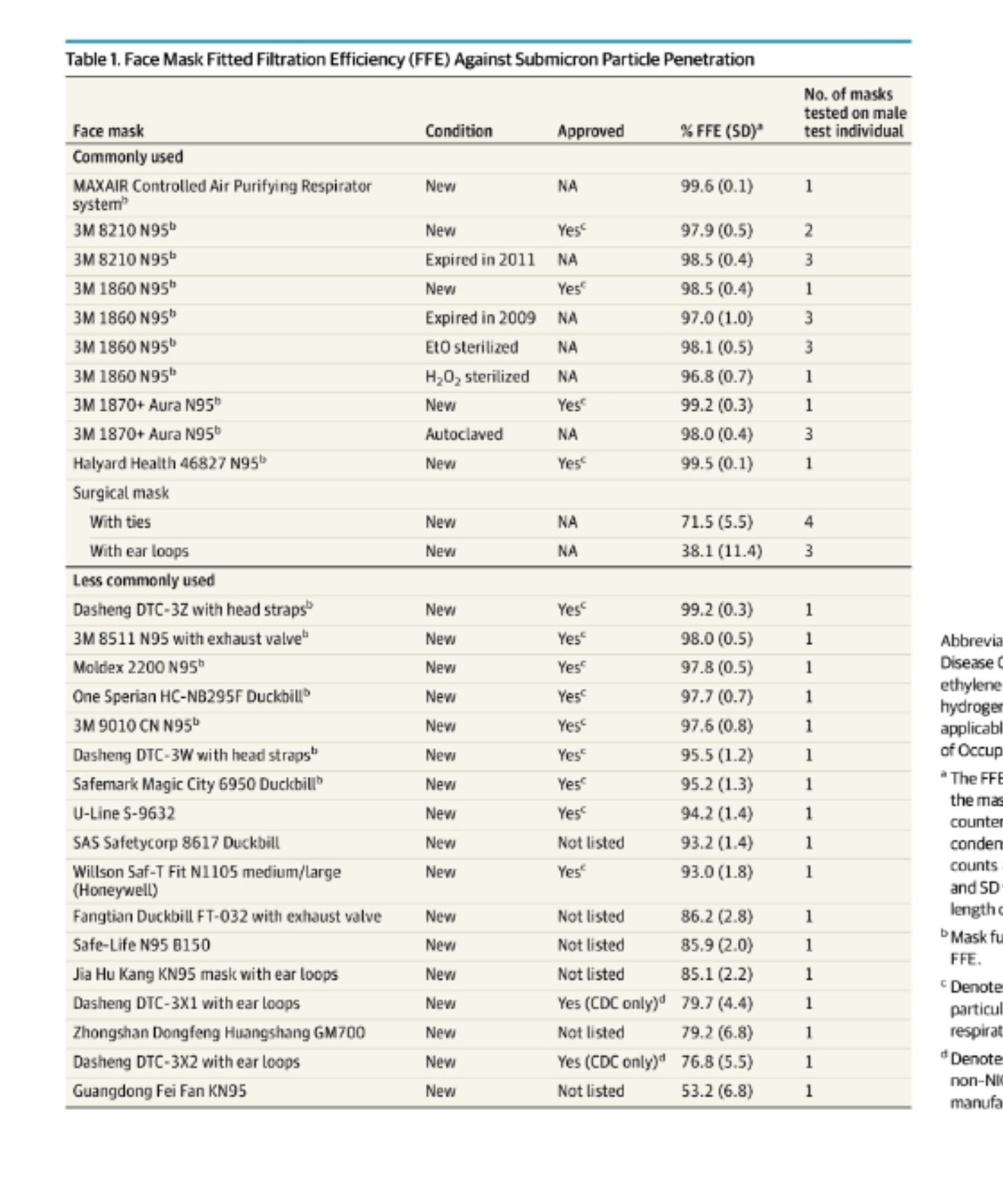
JAMA review of masks, August 2020
4. Where a high percentage of the local population tests positive, local authorities should consider – and have the ethical responsibility to – impose higher isolation measures like masks and public distancing. The threshold for mandates must be locally determined with public input, and explained – clearly, frequently.
This means you, anti-maskers!
5. Stress that surgical procedure masks are nearly as effective as N95 masks, blocking nearly as much aerosols and viral particles for both wearer and those around us. Medical providers and those with a high risk of prolonged close contact need fitted N95 masks, the rest of us don’t.
Single layer cut-up T-shirts and homemade masks, balaclavas or bandannas, aren’t very effective protection at all, either for the wearer or the people around us. N95 Masks with single valves are a money-maker, but not nearly as effective as surgical masks, even with an added filter layer.
8. Begin early prophylaxis with hydroxychloroquine/zinc and/or inhaled steroids for the willing & likely exposed.
REFERENCES
Treatment dosing (always allowing treating physicians who prescribe determine need & frequency of alternate doses & monitoring)
This isn’t a prescription!
Hydroxychloroquine: 400 mg. twice on day one then 200 mg. twice a day for either 5 or 10 days;
Azithromycin: 250 mg. tablet, 2 on day one, 1 on day 2 to 5;
Budesonide: unit dose via hand held inhaler or nebulizer twice a day. (I’m looking for references for this one. )
Zinc 150 mg. to 250 mg. a day indefinitely. (Best evidence for lozenges or syrup multiple times a day. See references.)
Vitamin D, 1000 IU a day, up to 4000 IU is safe
Vitamin C, No set dose, but extra will be excreted in the urine or feces, can cause diarrhea.
References
Journal of the American Medical Association review. Published August 11, 2020. (Free, with Tables)
CDC recommendation on cloth masks:
https://wwwnc.cdc.gov/eid/article/26/10/20-0948_article
John’s Hopkins recommendation:
Zinc:
https://www.uchealth.org/today/zinc-could-help-diminish-extent-of-covid-19/
Journal article on treatment for the common cold: https://www.acpjournals.org/doi/10.7326/0003-4819-125-2-199607150-00001
Hydroxychloroquine/azithromycin protocols
International Journal of Infectious Diseases (Henry Ford or Ashad report):
https://www.ijidonline.com/article/S1201-9712(20)30534-8/fulltext
https://www.ijidonline.com/article/S1201-9712(20)30600-7/fulltext
On synergistic effect of hydroxychloroquine plus steroids:
https://www.ijidonline.com/article/S1201-9712(20)30613-5/fulltext
Budesonide
Description of study in progress on treatment for loss of smell in patients without severe symptoms:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7370627/
Vitamin C safety:
Note: comments are off. Please comment on my Facebook page, Beverly Nuckols.
Edited 31/08/20 12:30 for mis-spellchecked word. BBN
Entire abnormal human genome in vaccine?
Quintessential anti-vaccine propaganda. The first sentence indicts the source, Mike Adams, the founder of “Natural News” and seller of food supplements like Organic Broccoli Sprout Capsules with a side of conspiracy.
Yet, that’s what they accuse the “cancer industry” of doing.
Finally, the accusations in the video have been rejected in court. This, in spite of the low requirements for vaccine injury compensation.
Edit 10:15 AM 10/07/2019: The MMR assay report from Corvelva is here. I’m skeptical about the “entire genome” supposedly found. Are they saying that all 23 chromosome pairs are present in each dose? BBN
HB 896 Abolish abortion in Texas

#HB896 @TxLeg
The Texas Legislature only meets for 4 months, every other year. Every session, several Bills are introduced that would regulate abortion in our State. Monday night, April 8,the House Committee on Judiciary and Civil Jurisprudence, chaired by Representative Jeff Leach, heard testimony on HB 896, authored by Representative Tony Tinderholt. HB 896 would change Texas law to treat elective abortion for what it is: the intervention intended to kill a member of the human species. The law would require that abortion be treated the same as a felony murder is treated by Texas law: “entitled to the same rights, powers, and privileges as are secured or granted by the laws of this state to any other human child.”
You can watch the testimony in the House Broadcast Archives.
Those of us who believe in human rights must decide whether laws can legitimately divide humans into two classes: those members if our species who are and those who are not human-enough to possess legal, protected (“inalienable”) human rights.
Yes, the law would create complications in a world that’s become accustomed to the act of elective abortion, “spare” human embryos, fetal research on aborted children, and arbitrary “choice” as to which babies live and which are susceptible (in New York State, for instance) to killing on the day before they become citizens by being born.
However, we know how to deal with those complications, because of lessons we learned in our Nation’s history of slavery and the abolishment of slavery. The lives and livelihoods of slave brokers, slave breeders, and slaveholders were disrupted by declaring slavery illegal in the United States, with penalties.
The (dreadful) Supreme Court Dred Scott decision about the status – the “inferior” humanity – of Black slaves has never been overturned by the Courts. In that 1850 ruling, Chief Justice Roger Taney stated that the Constitution affirmed that black slaves were not only property, but “beings of an inferior order” and that they and their descendents could never be citizens of the United States.
Ultimately, a Civil War and Constitutional Amendments 13, 14, and 15 were necessary to outlaw slavery and allow black persons, including former slaves and their children, to become citizens. The 14th Amendment also protected non-citizens, prohibiting laws which “deprive any person of life, liberty, or property, without due process of law; nor deny to any person within its jurisdiction the equal protection of the laws.”
A Constitutional Amendment may be necessary in this case, too, but I don’t think so, because of the way Roe v. Wade was decided.
Roe v. Wade is the Supreme Court decision that declared that there was a “right” to abortion under the Constitution. Justice Blackmun refused to
“. . . resolve the difficult question of when life begins. When those trained in the respective disciplines of medicine, philosophy, and theology are unable to arrive at any consensus, the judiciary, at this point in the development of man’s knowledge, is not in a position to speculate as to the answer.
“Man’s knowledge” has developed since 1973. Philosophers and theologians may still argue (as they do about the civil rights and personhood of neonates, the disabled, and the elderly) but the science is clear. Ultrasounds, MRI’s, and in vitro fertilization have all demonstrated when the life of human beings begins. Just ask the newest technician in the in vitro lab.
As a doctor, I deny that elective abortion is healthcare. I certainly deny that the baby in utero is a part of the body of the mother. It’s not logical to say that the embryo, then the fetus, is not the same organism that we call a baby as soon as he or she is born.
If nothing else, we now have evidence in the form of serial ultrasounds (US) and in vivo MRI’s that demonstrate that human life is a continuum that begins at fertilization.
Even 30+ years ago in training, I saw US used to follow an oocyte from just before ovulation, to the developing embryo in the uterus a few days later. We’ve all seen the US of children as they develop.

Just this month, a research article in the journal Developmental Cognitive Neuroscience reported on sex differences in functional connectivity of neural pathways in the brain, demonstrated by functional MRI of babies in utero.
Questions were raised by the Committee members and citizens alike about a possible death penalty for the felony murder of the unborn child, about women who are coerced into having abortions and whether or not the mother would be charged and subject to penalties.
Well, what penalty does the State impose for procurement of a contract to kill? What charges are brought against the mother who smothers her baby at birth?
It’s true that laws in Texas have never punished the mother who has an abortion. Part of that is out of compassion for the mother who is seen as a victim of circumstances. However, the main reason is that most laws regulating abortion have been passed under the legislation regulating medical practioners and technology, rather than as a civil or human rights issue.
In fact, abortion performed by the mother has always been treated as self-harm, like attempted suicide. But that custom was established before modern information about human embryology. It was long before medical abortion utilizing Mifepristone ( RU486) or methotrexate. We all know now that the mother is not killing a part of her body in an abortion and certainly not when she pays a third party to do it.
I believe that invoking the threat of the death penalty is a red herring. Our homicide laws recognize the right to kill in self defense (for the life of the mother) and mitigating circumstances such as mental illness and in cases of force and abuse by a third party, allowing for different degrees of homicide.
We don’t, however, allow euthanasia or eugenics in the case of born disabled children or give the mother the “choice” to kill by poisoning or distruction of the body of a child who becomes unwanted after birth.
Texas declared the child an individual before birth back in 2003, creating a penalty for third parties who cause the death of a child, except in the case of intentional abortion by a doctor or when the mother herself acts. There have been several convictions under the Texas Prenatal Protection Act.
In light of our expanded knowledge about human biology, it’s time for the Supreme Court to overturn Roe v. Wade and declare what Justice Blackmun deferred: life begins at fertilization and all humans possess human rights that should be protected by the State.
Maybe I’m tilting at windmills, but I would like to see Texas defy Roe v Wade and pass HB 896.
I’ve disabled comments on the blog. Please leave your comments on my Facebook page, “Beverly Nuckols.”
Scott Adams Jumps the Shark**
I enjoy Ben Shapiro’s Sunday Specials; one hour conversations with current thinkers and doers. I watched this week’s conversation with Scott Adams, the creator of the Dilbert comic with a bit of disbelief. (I watched on The Daily Wire, but it’s also available on YouTube.)
From approximately minute markers 29 to 45, Adams’ discription of his belief in the future (or existing) computer “algorithm” which will to decide future elections (“Trump is the last human President”), the denial of free will (but “I act as though” it exists), to turning toward the camera to repeat that “the end *always* justifies the means,” and finally to the idea that we live in a simulation of life that just seems like reality Adams displays a loose connection with reality accompanied by relatively sane inserts.
I love good science fiction and there’s no doubt that Adams is an intelligent man. But he’s not a great philosopher. I agree with Shapiro when he asks whether Adams is just trying to avoid God with his simulation. Just as some physicists posit multiple universes to explain ours, Adams requires multiple simulations.
Oh, well, if it makes you “happy,” Scott.
Reading Dilbert irregularly over the years, I’ve been repeatedly turned off by Adam’s anger and bitterness. Sometimes it just can’t be disquised as wit. Now I wonder whether the anger has affected his rationality: does he even know what or when he says something wrong or immoral?
Perhaps. Adams displayed physiologic changes consistent with stress: blinking more often and his neck reddened as the hour went along. Is he stressed at examining his beliefs or by lying – invoking hyperbole about hyperbole – about them? Or is he just stressed by thinking his thoughts through, out loud, in an effort to be witty and change Shapiro’s mind?
(**”Jumping the Shark” is a reference to going too far, indicative of lost relevance.)
Comments are disabled. Please post comments on Facebook.
Is there a solution to the current immigration emergency?
I’m following and responding to the news reports and conversations on Twitter and Facebook about the arrests and separations of alien families because I’m looking for a solution that will work and have fewest unintended consequences.
We can spend all day screaming our objections or justifications and playing political games based on what should have been done and when, in the past and present. Or, we can tell our legislators that we recognize the reality of the circumstances, today, and that we need to make immediate changes, followed by more measured steps.
We urgently need to:
1. Ensure that the very young are safe and nurtured. This is an emergency, because of the damage that we know tactile deprivation has on small children. No more claims that some institutional rule prohibits holding a toddler;
2. Make sure that no more children are “lost” and that even those who are separated can communicate with their parents.
(Hospital arm bands? Schlitterbahn and the Toob renters in my home town use similar bands. The tracking numbers could follow numbers on the bands and would not only work better with digitizing information
Would it be possible/permissible to use RFID and/or GPS?
Delta uses bar codes attached to each suitcase and can text me when my suitcase is loaded or unloaded on the plane. Last month, when I was on a cruise, ATT texted me that I wasn’t covered by their international plan as soon as I stepped on the ship, before the ship left the dock.);
3. Speed up the process of reuniting the families;
(This last will be enabled by the above, but will also require resources for the rapid setting up of family shelters for those awaiting hearings, and hiring personnel for those shelters and judges to hear the cases and lawyers to represent the asylum seekers.);
4. Streamline the process for approving or rejecting application for asylum at the ports of entry. (See above. This may be a useful job for civilians -paif or volunteer – and the National Guard after apprehension and/or initial evaluation by Border Patrol);
5. Fix the laws concerning detention of children separated from their parents, the right of application for asylum for anyone who manages to step on US soil, temporary worker permits that do not allow family to immigrate, and for immigration in general;
6. Continue to identify, arrest, and prosecute people who willfully violate our immigration laws;
7. None of this is dependent upon or contradictory to securing the Border. All of them are enhanced by increased security, however;
8. Stop the partisan game playing!
It should be made clear that our government will follow the law as written. Perhaps we can continue the ads Obama’s Administration is said to have used in Central America.
None of these should be done so that more people show up expecting immediate visas, green cards, or even healthcare and food stamps. They certainly shouldn’t believe that they have a right to immigration or to burden our social infrastructure and taxpayers.
Please comment on my Facebook page.
Edited numbering, BBN
Happy Birth Parent Day

- Google Images for “Baby Daddy” card
That lawsuit I wrote about yesterday would not only would put an end to Texas’ Medical and legal regulations on abortion – including informed consent, waiting periods, and sonograms – the plaintiffs go out of their way to redefine mother and father, too.
“”1 Most people with the capacity to become pregnant identify as women. Historically, both jurisprudence and public health data have focused on women when addressing reproductive rights and health. But there is an emerging recognition in the law and society more generally that not all people who may become pregnant identify as women. See generally Glenn v. Brumby, 663 F.3d 1312, 1316-19 (11th Cir. 2011)(holding, consistent with the weight of authority, that the Equal Protection Clause prohibits discrimination on the basis of “gender nonconformity”) (collecting cases); Robin Marantz Henig, How Science Is Helping Us Understand Gender, National Geographic (2017), https://www.nationalgeographic.com/magazine/2017/01/how-science-helps-us-understand-gender-identity/. The Constitution protects the rightof all individuals to end an unwanted pregnancy, regardless of gender identity.”
From the UK, we see the inevitable results in a time of identity and personal choice :
“Lawyers have told a judge that he had been biologically able to become pregnant but had legally become a man when the child was born.
“They say the transgender man wants to be identified as the child’s “father” or “parent” on a birth certificate.”
And, in Ohio:
“Explaining their unusual parenting arrangements, Amy said: “We went through a lot of fertility treatments, until we finally reached a point where we needed to make a decision as to whether we were going to do more medical intervention or if we were going to switch bodies. (emphasis mine)
“We were fortunate enough to have two uteruses. So, after a lot of thought and emotion and difficulties we switched to Chris.
“And while Chris lived as a man and didn’t feel female, he was willing to use his womb for the good of their family.”
Of course, neither Chris nor Amy could donate sperm. So, who is really — is there even — a father?
Or a parent, of either gender or any identity, who sees the child as his own person, human-enough to possess inalienable rights, rather than a political statement and a means to an end?
Existing tariffs, duty, and barriers to trade in Canadian law.
Current barriers on imports into Canada from the US affect dairy, wine, telecommunications like TV, cable, and broadcasting, and even software and “cloud” data storage.
https://www.export.gov/article?id=Canada-Import-Tariffs
In contrast, there are very few barriers to trade with Mexico.
(Edited to add the link to information on Mexico.)
Human-chicken hybrids in the lab
Nature reports on the creation of human-chicken hybrids using “embryo-like structures” in order to study human embryonic “organizer cells.”
, in an organized manner.
Response to criticism about Texas Advance Directive Act
I’ve been having a long Facebook discussion with representatives of organizations, people who claim that I support coercion and killing patients because I defend the Texas Advance Directives Act, 166.0046. (TADA).
I want to respond as fully as I can. ( I’m bandwidth deprived today and will gradually add more links when I reach better signals. See here, here, and here for more explanations from earlier WingRight posts. Links to the law, the press, and previous blog posts by others can be found in those articles.)
It was easy to follow this case. There was a video published by Texas Right to Life (TRTL), a lot of press, statements to reporters by family, lawyers, and TRTL staffers, as well as a couple of lawsuits. I spent the better part of two days once again reviewing the public records.
It
(Edited 03/11/18 for typos, to add a link, and to clarify points originally made on Facebook in a long debate. BBN)
When the Truth is Crazy
Excellent op-ed in the Wall Street Journal, “When the Truth Is Crazy.”
This is a line I may find occasion to quote in the future:
“Failure to conform, in any society, is treated in casual parlance as prima facie evidence of insanity. And the media, in any society, exist at least partly to enforce such conformity, not truthfulness.”
The author, Holman W. Jenkins, Jr., goes on to make the point that the Dems shot themselves in the foot by not exploiting the fact that Trump was himself a Dem or Dem-leaning until recently – or, even, perhaps working with him to pass the infrastructure funds.
My theory about the Russia accusations is that the Wassermann-Schultz IT scandal (an “unbiased” review by the Washington Post, here, and the Daily Caller’s more thorough review, here) as well as Podesta’s “password” password controversy (see the UK’s Guardian coverage, here) , along with the cheating to defeat Bernie Sanders, was serious enough to necessitate distraction. And we all know that there’s quite afew irregularities in the Comey and Lynch, etc., cover-up of Hillary’s illegal server and “carelessness” with government security.
(I couldn’t come up with a better title than Mr. Jenkins’ own.)
Personhood “TBD”
“To Be Determined,” or the Schrodingder’s cat* version of human rights.
Does the possession of inalienable human rights depend on unknown future facts? Can the moral worth of a human being be determined by the actions of another human being – or by fate, the available and utilized medical technology?
Sherif Girgis discusses the theory of Princeton philosopher, Elizabeth Harman, in today’s Public Discourse. The professor’s view that abortion is – or may be – a neutral act has been the subject of discussion since she appeared in the YouTube video, Philosophy Time, produced by actor James Franco and Eliot Michaelson.
Besides the obvious problems pointed out by Girgis of defining “consciousness” and the TBD “kind” of a human fetus, there are other problems.
First, any concept of “inalienable” human rights would need to be discarded. There goes the Declaration of Independence and the basis of the United States Constitution.
In addition, Professor Harman’s theory would presumably allow the use of bodies of the human species for the benefit of humans with “moral worth,” as long as those bodies are never allowed to become conscious. This is the current practice of researchers using embryos, including those created for the purpose of manipulation and destruction.
But there’s nothing in this philosophy to prevent the intentional manipulation of a human body for research or to benefit others, as long as the body is never allowed to develop consciousness. Continual sedation or mutilation of the brain from the beginning – before consciousness – would prevent the development or acquisition of moral worth and rights.
In the process, “human” rights would cease to exist. The actions of others, laws and location and the potential use of technology would finally determine who is human enough to possess the right not to be killed. (Forget the right not to be “enslaved.”
What happens if (as Girgis proposes) the abortion itself is aborted or fails? Or if the brain isn’t damaged sufficiently to prevent consciousness?
Forget about opening the box: don’t put humans in there in the first place.
*I saw this analogy on a Facebook thread, but thought the same thought before I stole it.
Edited to correct my misspelling of Dr. Harman’s name.
Latest story on ethical stem cells in Texas
Last week, in a story about another baby boy, there was a a beautiful memorial to the “Bubble Boy,” David Vetter, too.
The story in the Houston Chronicle is also a tribute to the doctors and parents who keep immune compromised children alive while waiting for the cure or treatment to take effect.
My granddaughter’s mother is one of those heroes, helped by doctors and nurses, my son and an extended family of friends. (I can’t help my prejudice that gives the mother most of the credit.) And then, there was a baby boy and his generous mother.
I told Roni’s story to the Texas Legislature back in 2007 and 2006. An anonymous baby boy and his parents saved Roni’s life in 2001.
In addition to a very low white blood cells count, her bone marrow didn’t make enough red blood cells or platelets, either. She’s healthy and well, today, after one of the first cord blood bone marrow transplants in the world at the age of 15 months.
Although no matches were found for Sebastian, the baby in today’s story, Texas has a strong system for the registration of both bone marrow and umbilical cord blood donors. The Texas Cord Blood and MD Anderson Cord Blood Centers collect, store s and manage the distribution of donated cord blood collected at birth from moms and babies all over the State.
Families who store their baby’s cord blood privately are very unlikely to ever need it, except when there’s a known problem. The odds are less than 1:200,000. But if they donate to a public bank, the blood is much more likely to save a life and/or be used in life-saving research.
Bravo to all the parents and caregivers in children’s lives and prayers for Sebastian. There’s a Go-Fund-Me account for Sebastian’s expenses, if you are interested.
Edit: there’s a wonderful update: Sebastian was able to go home!
Human cloning fable doesn’t justify abortion.
Sigh . . . There are still people out there trying to justify elective abortion of healthy babies in healthy mothers by claiming that the embryo is nothing special, since liver tissue is alive when it is harvested for transplantation and ” . . . a skin cell contains DNA that could be implanted into a human egg and be developed into a baby.”
That hypotheticals is, at this time, just that. No one has yet been able to clone humans beyond a very early blastocyst. In some way, these embryos don’t function well enough to maintain organized cell division, development and growth.
However, even if cloning a human were possible, that new human life would not begin at the harvesting of either the skin cell, the liver tissue or the oocyte destined to be enucleated. Just as with gametes in vivo, those cells are end-stage specialized cells that do *not* actually have the potential to be other types of cells – much less a new human – without fertilization or the manipulation that scientists might someday be able to discover.
The natural, in vitro, or someday-maybe cloned human life begins at fertilization or not-yet-achieved generation of functional clones. Each are – or would be, in the case of the hypothetical – verifiable by observing the organized cell function, development and division in the embryo, driven by the nucleus of the new organism. Intentional, interventional abortion ends that organized development and growth, causing the death of the organism.
I’m sure my explanation won’t stop those who really, really, reeeally want to abort unwanted humans from using junk science to justify killing humans. Most likely, they will just go back to those long essays discriminating between which humans are human-enough.
Jihadist courage
Bioethicists and transhumanists – and I – have long speculated on the ability and usefulness of drugs to enhance performance. However, assassins, murderers and the subgroup that are the jihadists, have a completely different goal for their “enhancement.”
“Captagon — a synthetic amphetamine-based pill — is considered the drug of choice for Islamic State fighters in Syria, Iraq and, now it seems, Paris.
‘When French police raided a hotel room at Alfortville, south-east of Paris, last week they found a stash of syringes, needles and plastic tubing.” (from http://www.abc.net.au/news/2015-11-24/captagon-the-drug-that-kept-the-paris-attackers-calm/6970464 )
Hat tip to BioEdge
Detention, boxcars and “papers”
Please read the link – or at least the entire quote I’ve pasted here – before commenting.
The immigration debate and its ability to divide the Republican Party and split the Conservative vote is not new. Here’s a commentary about the dispute in light of the 2012 Presidential election, written in 2011. (Scroll down the page to “On Immigration,” Saturday, May 21, 2011.)
Dr. Jerry Pournelle has served our Nation in many capacities (including serving in the Army during the Korean War), but he’s probably best known, to those who know his name at all, as the author of Science Fiction written from a conservative, libertarian-leaning viewpoint. I strongly recommend his essays, including this one from 2011:
“We aren’t going to deport them all, and no Congress or President will do that, nor could even if it were thought desirable. The United States is not going to erect detention camps nor will we herd people into boxcars. We can’t even get the southern border closed. Despite President Obama’s mocking speech, we have not built the security fence mandated a long time ago. We probably could get Congress to approve a moat and alligators, although there are likely more effective means. We can and should insist on closing the borders. That we can and must do. It won’t be easy or simple, but it’s going to be a lot easier than deporting 20 million illegals. Get the borders closed. We can all agree on that.
“That leaves the problem of the illegal aliens amongst us. We can and should do more to enforce employment laws; but do we really want police coming around to demand “your papers” from our gardeners and fry cooks and homemakers?”
This is not a trivial point. I advocate for the necessity of identifying illegal aliens and would prefer that the process begin in the country of origin. However, in practical terms, how would the “Maria” Dr. Pournelle describes, who was brought here as a child, “begin the process?”
Defense and security requires that we secure the border and that we identify as many who are here illegally as possible. A first step would be to better track people who enter on Visas: what are all those computers at border entry spots for?? We should also cease the fiction that our schools don’t know which families with children are undocumented. We should hold employers accountable, but be very careful about instituting new government papers and government computer lists of eligible workers.
We must determine common ground for the sake of success. As pointed out four years ago by Dr. Pournelle, errors will be used against us, with the hard cases like “Maria” will be splashed across media and social networks. Without common ground, and with emotional demands to “deport them all,” we’ll still be debating this four years from now. And our citizens – and the illegal aliens – will remain at risk from the violent and criminal, if not from the terrorist.
“Duty” to use human tissue?
 We should at least have as much care for the donation of tissue from aborted human fetuses and embryos as we do for the donation of organs from those killed by capital punishment. Both scenarios involve purposeful intervention to cause death and the collection of tissues, at least, must be carried out by licensed and regulated medical personnel.
We should at least have as much care for the donation of tissue from aborted human fetuses and embryos as we do for the donation of organs from those killed by capital punishment. Both scenarios involve purposeful intervention to cause death and the collection of tissues, at least, must be carried out by licensed and regulated medical personnel.
Robin Alta Charo (a law and ethics professor at the University of Wisconsin) has an opinion piece in this week’s New England Journal of Medicine, “Fetal Tissue Fallout.” in which she claims that society has a “duty” to use tissues harvested after elective, intentional abortions.
I object to the idea that society has a “duty” to make use of the end products of either procedure. Both scenarios involve purposeful intervention to cause death by licensed and regulated medical personnel, making those of us who vote for the legislators who write laws complicit in the actions, at least remotely. Under a strict philosophy of ethics based on the protection of inalienable rights, each act should be weighed individually and should only be carried out when the one killed is a proven danger to the life or lives of others.
Robin justifies her elevation of the use of fetal tissues after elective abortion to that of a “duty” by citing past benefits of research using fetal tissues. She is more political and names past Republican supporters in an earlier op-ed, published in the Washington Post on August 4th.
Yes, society has benefited from these tissues. However, that picture at the side of this post depicts Dr. Frederick Robbins, one of the scientists who utilized fetal tissue in the 1950’s development of the Salk polio vaccine. Dr. Robbins is depicted smoking at work in the laboratory, while handling test tubes without gloves. We know better than that, now. Isn’t it time that science and medicine researchers catch up with our knowledge that the human fetus is a human being from the moment of fertilization?
Where are the Ethics Review Boards that monitor for the unethical behavior we’re hearing about in the videos from the Center for Medical Progress?
In 2013, the science journal, Nature, published an article covering the history and evolution of informed consent and compensation for donors of human tissues, including the fetal tissue culture, WI-28. Ms. Charo was quoted as supporting monetary compensation:
But, says Charo, “if we continue to debate it entirely in legal terms, it feels like we’re missing the emotional centre of the story”. It could be argued, she says, “that if somebody else is making a fortune off of this, they ought to share the wealth. It’s not a legal judgment. It’s a judgement about morality.”
Yes, “It’s not a legal judgment. It’s a judgement about morality.”
Convergence – politics, economy, philosophy
Pretty much whatever our politics, our client (sorry) lies in the past. Maintaining the programs of the Great Society? Returning to the vision of the Founders? Addressing as #1 priority the debt mountain we have built? Each of these is meritorious, and wherever our political lines lie for most of us each of them features. Point is not that they are misplaced priorities. It is simply that they hail from yesteryear. Left and right are stumbling into the future as their gaze is fixed on the past. (“How to bridge the Continental Divide; moving Camp David to the Valley; please, pols, start Asking Tomorrow’s Questions.” Nigel Cameron, President and CEO, Center for Policy on Emerging Technologies. )
“The shrill universal cry that we are at a “tipping point” is correct, but not as they would have us all believe, the tipping point that is fast approaching has to do with the old political and legal superstructures being torn apart from below by this powerful, complex, emergent force of scientific and technological evolution now unleashed. Reactionaries are doing all they can to bamboozle gullible people into helping support the status quo, to prop it up, which is unfortunate.” (Quote from C. James Townsend, in “The Singularity and Socialism, An interview with C. James Townsend” by BJ Murphy on Murphy’s “Serious Wonder” blog, distributed by the newslist/email of the Institute for Ethics and Emerging Technology.)
This week, two email subscriptions I follow converged with a common warning that government is reacting to and protecting the past. Each, one from the right and one from the left, urge politicians to allow innovation and technology to frame the debate on the economy.
Regulate anti-vaccine docs?
 We may not ever solve the problem of an irresponsible tabloid press and sensation-seeking media, since the freedom of speech is too important to infringe. But we do have power over those we license as physicians.
We may not ever solve the problem of an irresponsible tabloid press and sensation-seeking media, since the freedom of speech is too important to infringe. But we do have power over those we license as physicians.
Dr. Walt Larimore enters the vaccine debate in his blog, not by suggesting forced vaccination, only the regulation of physicians. I wouldn’t support the recommendation without some leeway — I’m certainly not going to approve of every vaccine without a time trial in this very diverse lab that is the United States.
However, Dr. Larimore and his guest author, Dr. Russell C. Libby, are right to raise the ethical and medic0-legal responsibility of physicians who are licensed by the State and who advocate against good science and medical standards.
From the article:
“State medical boards must decide if the actions of healthcare practitioners who advocate against vaccination and undermine the public health efforts of their communities warrant investigation and intervention. There are a number physicians and other licensed healthcare professionals who trivialize and discourage immunization, whether it be for philosophical, financial, or self-promotional reasons.
“When the patients they influence contract preventable disease and have bad outcomes or they cause the spread to a vulnerable population, they should be held liable for malpractice. If it is in the midst of an outbreak or epidemic, medical boards need to sanction or suspend licenses.”
I’ve spent quite a bit of time — especially over the last week – attempting to educate interested people (including a family member) about the safety and usefulness or efficacy of vaccines. My motto for these arguments has always been that, “Truth will out,” and, “If we’re right, we should be able to teach and convince.”
However, within the last week, an irresponsible Texas radio host trotted out the discredited and un-licensed doctor who fabricated the MMR/autism fraud and a Canadian newspaper published a hit piece on Gardasil. (You can find them easily on Google – I won’t give them “hits” from my page.)
When licensed physicians – men and women who should know better – spread demonstrable lies, even after being found guilty of fraud or when demonstrably spreading harmful misinformation, there should be consequences.
I say “fertilization,” you say “conception”
Forty years ago the words “fertilization” and “conception” meant the same thing to doctors, lawyers, and embryologists alike: the joining of the 23 chromosomes in the sperm with the 23 chromosomes in the oocyte (“egg”) to form a new complete, unique human organism. “Contraception” was defined as any method that worked before the existence of the embryo by preventing fertilization. These were the hormonal treatments and devices that prevent ovulation of the egg and condoms, diaphragms and sterilization that serve as “barriers” between the sperm and egg. Drugs and devices that may or may not end the life of the embryo after fertilization were legally and correctly called “abortifacients.”
However, legalized abortion and the ability to accomplish fertilization through in vitro methods led to new legal definitions of “pregnancy” and “conception” as beginning at implantation rather than fertilization. Even in vivo, healthy human embryos in healthy mothers were deprived of legal protection as human beings for at least the first 5 – 10 days of their lives, the window of opportunity for implantation when the developing embryo grows to hundreds of cells organized in 2 or 3 recognizable tissue layers and interact with the mother’s body in ways that may affect the timing of birth or risk of diabetes and other health concerns. Possible abortifacients that work after fertilization but before implantation were redefined as “emergency contraception.”
In spite of what you may have heard on the news, the June 30, 2014 Burwell v. Hobby Lobby decision by the Supreme Court of the United States (SCOTUS) didn’t deny birth control for anyone. Everyone may still purchase his or her own FDA-approved birth control. SCOTUS simply ruled that the government can’t force some employers to buy things that they believe are immoral.
In fact, Hobby Lobby only asked to be exempt from purchasing insurance plans that paid for specific drugs and devices used for “emergency contraception.” Before the passage of the Affordable Care Act (“ObamaCare” or ACA), the company purchased insurance that included true forms of contraception, including,
- Those that prevent ovulation by preventing the normal ups and downs of the hormones estrogen and progesterone, such asBirth-control pills with estrogen and progestin (“Combined Pill”),Birth-control pills with progestin alone (“The Mini Pill”),Birth control pills (extended/continuous use), Contraceptive patches, Contraceptive rings,Progestin injections, andImplantable rods
and
- Those that act as “barriers” to fertilization by preventing the union of sperm and egg: Male condoms, Female condoms, Diaphragms with spermicide, Sponges with spermicide, Cervical caps with spermicide, Spermicide alone, Vasectomies, Female sterilization surgeries, and Female sterilization implants.
The problem is that regulations written by the Obama Administration mandated that all insurances pay for all pregnancy “preventatives” approved by the FDA, including drugs and devices that may function after fertilization to end the life of the new human embryo:
- Pills that mainly delay ovulation but may impair implantation and development of the placenta if fertilization takes place, such as over-the-counter Plan B and generic levonorgestrel tablets, and ella, which requires a prescription, and
- Devices that mechanically and hormonally make the uterus inhospitable to implantation by the embryo, such as intrauterine devices like the copper-T, Mirena, and ParaGuard. These are inserted up to 5 days after unprotected intercourse to prevent implantation and then left in place to prevent fertilization and implantation for as long as 5-10 years.
Although the words we use do not change the fact that the human embryo is the same human life before implantation as after, they can change his or her legal status.
Do you feel male, female, American, other?
 Can’t help worrying that I might be prosecuted for hate speech for insisting that physical evidence matters, but . . . if a person can demand a corrected birth certificate based on his/her subjective feelings about his/her gender, why can’t an illegal alien access his/her own new birth certificate if they feel American?
Can’t help worrying that I might be prosecuted for hate speech for insisting that physical evidence matters, but . . . if a person can demand a corrected birth certificate based on his/her subjective feelings about his/her gender, why can’t an illegal alien access his/her own new birth certificate if they feel American?
And if it’s all in our heads, why make Medicare pay for surgery?
The same month that the American Medical Association voted that the physical body is irrelevant to gender, President Obama uses his pen to award physical privileges to those people who claim/decide/are born to be transgendered. But he’s doing it very, very quietly.
The latest wins came this month, when the Office of Personnel Management announced that government-contracted health insurers could start covering the cost of gender reassignment surgeries for federal employees, retirees and their survivors, ending a 40-year prohibition. Two weeks earlier, a decades-old rule preventing Medicare from financing such procedures was overturned within the Department of Health and Human Services.
Unlike Obama’s support for same-sex marriage and lifting the “don’t ask, don’t tell” ban on openly gay troops, the White House’s work to promote transgender rights has happened mostly out of the spotlight.
Some advances have gone unnoticed because they also benefited the much larger gay, lesbian and bisexual communities. That was the case Monday when the White House announced that Obama plans to sign an executive order banning federal contractors from discriminating against employees on the basis of their sexual orientation or gender identity.
In other instances, transgender rights groups and the administration have agreed on a low-key approach, both to skirt resistance and to send the message that changes are not a big deal, said Barbara Siperstein, who in 2009 became the first transgender person elected to the Democratic National Committee.
New Braunfels Republican Women mentioned on Alex Jones’ Infowars
 We’ve made it to the big time, Ladies! via » Web Filtering Company Launches Purge of Libertarian, Conservative Media Alex Jones’ Infowars:
We’ve made it to the big time, Ladies! via » Web Filtering Company Launches Purge of Libertarian, Conservative Media Alex Jones’ Infowars:
Other sites besides Infowars.com have also been miscategorized by Blue Coat.
In the past, the company also labeled New Braunfels Republican Women, the web site of conservative commentator Carolyn Gargaro and Reunion Ministries as “pornography.”
To be fair, at one time there was a pornography site using the initials as NBRW. You can see our website at NBRW.com and our Facebook page is here.
Best of the Web Today: The Lois Stretch – WSJ
Not only are the emails lost, but they hoped the notice would be, also:
Camp notes that the IRS decided to “bury” the claim of lost emails “deep in an unrelated letter on a Friday afternoon.” He isn’t kidding. It appears on the 15th page of the document, which is actually the seventh page of the first attachment to an eight-page letter, addressed to Sens. Ron Wyden of Oregon and Orrin Hatch of Utah, respectively chairman and ranking Republican of the Senate Finance Committee.
The IRS asserts that it has “determined that Ms. Lerner’s computer crashed in mid-2011. . . . The data stored on her computer’s hard drive was determined to be ‘unrecoverable’ by the IT [information technology] professionals.” The agency further claims to have “confirmed that back-up tapes from 2011 no longer exist because they have been recycled.”
via Best of the Web Today: The Lois Stretch – WSJ.
And there’s more:
IT professionals from outside the administration say the Lois Stretch is quite a stretch, too. Norman Cillo, identified as “an Army veteran who worked in intelligence and a former program manager at Microsoft,” tells TheBlaze.com that if the IRS is telling the truth, it means the agency is “totally mismanaged and has the worst IT department ever.” According to Cillo, there should be multiple backups, on server hard drives as well as tape.
Health record app for Google Glass developed by Drchrono
Cool! Security will need to be tight, though.
Goo
gle Glass was put to work as part of a system involving a QR code posted on the doorway to each patient’s room and software that can read the code and call up the record of the patient. Dr. Horng noted how each second counts in a hospital environment and fast access to timely information can be life-saving; Horng also said he wanted to use technology in a way that kept doctors in front of patients, not screens, away from the computer and back to the bedside
via Health record app for Google Glass developed by Drchrono.
3D Printed Titanium Hip Combined with Stem Cell Graft Implanted Into UK Patient
Too cool!

A machine lays down the titanium for the false hip, dot by dot, line by line as with a printer. In addition, the docs used the woman’s bone marrow stem cells to aide in healing.
3D Printed Titanium Hip Combined with Stem Cell Graft Implanted Into UK Patient.
A Penguin in XP’s Clothing | Malwarebytes Unpacked
I’ve used Malwarebytes to protect my PC from viruses, worms, and other Internet vermin for years and have never had a problem. (There’s a free version, but consider paying to keep them alive.)
Malwarebytes’ blog, UnPacked, is also promising protection to those of you who are still using Windows XP and understands the problems of switching to Windows 8 for some users:
Rest assured Malwarebytes will continue to offer support for XP, to assist users who find themselves in this unfortunate position.
Many readers of our blog are also the familial tech support, and trying to migrate grandma to Windows 8 might not only be an expensive affair but also a potentially traumatic experience. Windows 8 is proving to be … challenging.
One of my family members went back to his laptop with the broken hinge and wobbly screen rather than switch from Windows 7 to 8, so I can imagine there are many, many who won’t like to jump even more evolutionary leaps.
The rest is a description of switching to another sort of code, Linux Mint, that can be made to look and act like a (safer version of) Windows XP. I probably could do it with a lot of coffee and some new cuss words, but anyone with a genuine problem with switching operating systems would most likely need some help from someone more tech savvy.
The important message is that Malwarebytes will protect your computer, even if you won’t or can’t switch
NEJM “I want” ethics
In the Abolition of Man, C.S. Lewis notes that, “When all that says ‘it is good’ has been debunked, what says ‘I want’ remains.”
Last week, the New England Journal of Medicine published a “Perspectives” column, “Life or Death for the Dead Donor’s Rule?,” in which the authors illustrate Lewis’ point with their redefinition of non-maleficence to better serve a re-defined autonomy.
They would convince us that there is no harm in hastening the death of a dying patient even by intentionally causing it if he or his surrogates ask. They ignore a 2500 year old First Principle of Medical ethics,focused on the health of the patient in front of us: “Cure when possible, but first do no harm, ”
Autonomy, like all rights, is a negative right: the patient has the right to refuse invasive medical interventions that will harm him or that he does not want. Patients and surrogates, if they can compel the use of medical skills and invasive technology, can only do so for the medical benefit of the patient himself.
Illogically, in these times of reducing costs, the authors would have us consider taking a patient from the ICU to the OR “and then take him back to where life support would be withdrawn.” The return to the ICU is nothing but our own “medical charade.”
The Abolition of Man can be read online, here, or you can buy the Kindle version at Amazon.com.
I want to thank Nancy Valko, who runs an email list covering a range of traditional ethics issues, her email alerting me to this editorial.
Compromise or computers: ObamaCare delay inevitable
“But in some situations, you may see a redefinition of what ‘start’ means.” (Wall Street Journal quoting Obamacare consultant.)
President Obama and Democrats everywhere should be grateful to the Republicans for saving them from a huge embarrassment. Instead, the Dems continue to dig in, escalating their claims to have won a mandate on ObamaCare in 2012, in spite of the fact that the Republicans won enough seats in the House of Representatives to secure a strong majority.
House Republicans passed a new Continuing Resolution that compromises on Obamacare, by changing from refusing funding altogether to setting up a one year delay. Included in the Bill is a measure that would ensure that our military is paid in the event of a shutdown. The Bill also repeals the 2.3% tax on medical devices and the mandate that business owners with religious objections buy insurance that includes controversial “free” contraception.
The Wall Street Journal, in addition to reporting the redefinition of “start,” outlines the many ways that the Federal and State exchanges are not ready to launch Obamacare on October 1:
In the District [of Columbia], people who use the online marketplace will not immediately learn if they are eligible for Medicaid or for subsidies.
In Oregon, people will not initially be able to enroll in an insurance plan on the Web site.
In Vermont, the marketplace will not be ready to accept online premium payments until November.
In California, it could take a month for an insurer to receive the application of someone who applies for coverage on the exchange on Oct. 1.
. . . But as the launch nears, more delays are occurring. On Thursday, the administration announced a delay in the online shopping system for small businesses and confirmed that the Spanish-language site for signing up for coverage will be delayed until mid-October. Earlier in the week, officials said Medicaid applications will not be electronically transferred from the federally run exchange to states until November.
Just take care of the patient
 What causes a frail elderly person to become a patient in the hospital and can we do something in the home to prevent that event? What causes some people to develop chronic illnesses and can other people intervene to prevent the consequences of those illnesses?
What causes a frail elderly person to become a patient in the hospital and can we do something in the home to prevent that event? What causes some people to develop chronic illnesses and can other people intervene to prevent the consequences of those illnesses?
What if healthcare reformers asked these questions rather than focusing (or appearing to focus) only on costs? Better yet, what if they recognized the system changes that work, rather than insisting that all doctors must become employees of mammoth organizations, touting the business opportunities inherent in expensive, user-unfriendly electronic medical records and/or forcing an even more expensive change from the 5-digit medical diagnosis codes in ICD-9 to the 7-digit ICD-10 codes?
The source for the graph above is a report by the Oliver Wyman Healthcare Innovation Center, reviewed in Forbes Magazine last January by author Dave Chase. Yes, 5% of patients are responsible for 45% of the costs. What works to lower costs? Taking care of the patient:
In 2008, when physicians from CareMore, an independent medical group based in Cerritos, California, heard news reports of a brutal heat wave, they began contacting their elderly emphysema patients. Physicians worried that the scorching heat would drive their at-risk Medicare Advantage patients to the emergency room. So when patients said they had no air conditioner, the physicians purchased units for them. The theory was that the roughly $500 cost paled in comparison to the cost of an emergency-department admission. As it happened, this non-medical “intervention” kept CareMore’s patients out of the hospital. But if they had needed to go and lacked transportation, CareMore would have offered a free ride.
CareMore has an expansive, counter intuitive approach to healthcare. The group fends off falls by providing patients with regular toenail clipping and by removing shag rugs—a common household risk for the elderly. Patients engage in iPhone conference calls with healthcare professionals and are remotely monitored with devices that feed data automatically to doctors; for example, patients with congestive heart failure are given a wireless scale that reports their weight on a daily basis—a key step in preventing hospitalization. They have singing pillboxes that chime when it’s time to take medications.These unusual tactics produce enviable outcomes: CareMore’s hospitalization rate is 24 percent below average, hospital stays are 38 percent shorter than average, and the amputation rate among diabetics is 60 percent below average. Overall member costs are roughly 18 percent below the Medicare average.
The electronic medical record helped CareMore identify patients at risk, but the EMR is a minor tool compared to the minds of the innovators who recognized the real problems and acted in the best interest of the patients.
Click here to get your “Choose Life” license plate

Rick Perry RickPAC
Yes, I'm still for Governor Perry!
RickPAC
SiteMeter
