WingRight
Medicine
Maternal Morbidity with Premature Rupture of Membranes <24 Weeks
Because of the recent Supreme Court ruling, Dobbs vs. Jackson Women’s Health Organization, that overturned Roe v. Wade, misinformation has been spreading online and in public forums about the risk of maternal morbidity and mortality to mothers after premature rupture of membranes at less than 24 weeks or in the second trimester, which occurs in 0.3% to 0.4% of all pregnancies. The misinformation infllates the risk and usually tells of doctors’ hesitancy to treat due to fears of legal consequences.
In April, 2022, the American Journal of Obstetrics and Gynecology (AJOG) published an article, “Maternal morbidity after preterm premature rupture of membranes at <24 weeks’ gestation,” by Sklar A, Sheeder J, Davis AR, et al.
On average, there’s a greater risk in watch & wait. A day or 2 of careful conservative observation is much different than 14 days.
If you’re interested, here’s my review of the article Free! It costs $39 to read this whole thing, if not a subscriber.
We knew the risk difference for later gestations from past research. There have been a few studies describing the risks of maternal morbidity from premature spontaneous rupture of membranes (PROM) before 24 weeks, but the numbers were small & excluded women who chose termination of pregnancy.
In this retrospective cohort study – a chart review – from 2011 to 2018 at 3 hospitals, the review of 350 charts were randomly selected from an original 6747 potential cases to include. Of that 350, 208 were eligible, with women who spontaneously delivered within 24 hours excluded from the study, along with women with chorioamnionitis on initial presentation, fetal abnormalities, or PPROM after an invasive uterine procedure like amniocentesis.
Women who chose exprctant management (EM) but later decided to terminate the pregnancy were counted with the EM group.
Both induction of labor and d&e were included in the termination of pregnancy (TOP) cohort. Although the article describes the difference in the possibility of fetal survival, the outcomes were combined. This was noted as a weaknes in the article.
[My note: The prep for the induction is either a 1-2 day outpatient process for the d&e (with symptoms much like early labor), or an emergency manual dilation in the OR (with shorter preps having more risk to the integrity of the cervix).]
51.9%, 108 women, chose EM & those tended to be farther along in their pregnancies (mean gestational age 21 6/7 weeks vs 18 6/7).
2/3 of the TOP were labor induction & 1/3 d&e.
42 babies, 38%, of the 108 EM, survived to discharge. 15% of these mothers had no maternal morbidity, 37% of the group had both fetal demise & maternal morbidity. Composite morbidity was 60%.
All of the 100 TOP fetuses died. Maternal morbidity was 33%.
Political, purposeful lies (Francis Collins & Anthony Fauci)
I’m still researching , but so far, I’m disappointed by what I’m finding. It’s enough to make me, a conspiracy-denier, to begin to suspect that there really were multiple conspiracies, at least to control the public conversation.
The shame of Dr. Francis Collins, Director of the NIH, & his emails to Dr. Anthony Fauci about the Great Barrington Declaration, as reported in the Wall Street Journal:
““This proposal from the three fringe epidemiologists . . . seems to be getting a lot of attention – and even a co-signature from Nobel Prize winner Mike Leavitt at Stanford. There needs to be a quick and devastating published take down of its premises,” Dr. Collins wrote. “Is it underway?””
This is politics, not science.
Remember how the community seroprevalence/infection rates were disputed? Or the mandates that forced long term care facities – nursing homes – to accept infected patients, even though everyone knew that the facilities weren’t able to isolate the vulnerable or even protect staff?
Don’t expect anyone to be held accountable. Neither the US Department of Justice nor State prosecutors, at least in New York, appear set to continue investigation, much less charge those responsible.
I don’t expect much fallout about the US CDC’s sponsorship of – and Fauci’s dishonesty in testimony to Congress about – viral “gain of function” that quite possibly led to the creation and escape of the “novel Coronavirus” from the lab in Wuhan, China. Instead, the debate is used to divide the political Left and Right, not to discover the truth.
For a comprehensive discussion about the debate and the science, I recommend a video podcast from Lex Fridman, an MIT Ph.D., in conversation with Dr. Jay Bhattacharya – one of the original three “fringe” epidemiologists. Dr Fridman also interviewed Dr. Collins, but that was before the “takedown” emails were revealed.
Biden to Ask OSHA to Mandate Vaccines at Businesses With 100 or More Workers
A primary tenant of Western medicine is that people have the right to refuse medical treatment. President Joe Biden has ignored this tradition, the First Principle of Medical ethics (“First, do no harm”) and the Constitution of the United States.
In medicine, there’s a huge ethical difference between forbidding intervention and not only forcing individuals to comply, but forcing third parties like employers and medical personnel and administrators to intervene by mandating the involuntary breaching of bodily integrity.
The rare cases in contradiction are treatment of tuberculosis and psychosis where it’s proven that patients are an imminent danger to others, not just themselves. This infection can not rise to that level of threat.
There is a history consistent with quarantines – but only of the contagious or suspected contagious.
It’s an egregious violation of human rights to force invasive medical treatment on the unwilling except in emergent, extreme circumstances.
Long Post Reviewing COVID19 Myths
I’m often asked to comment on medical issues by friends. I’ve been having a Messaging conversation with a libertarian friend about what I consider myths. Here’s a loooong post, based on that conversation. I’m not linking to his reference videos, but you can search for them (or ask on my Facebook page) if you really want to give them the “clicks.” Comments should also be made on Facebook. (Keeping comments more public as well as trying to avoid “blog-pimping.”)
The problem I’ve seen is mixing criticism about policy (politics) errors from the actual science. It’s important to separate the science myths from the evidence for science facts. This “ZDoggMD” (Zubin Damania, MD) video is a good place to start for an overview. https://youtu.be/v8RpPeXCySw
As is this one, between Dr. Damania and Dr. Mike (Mikhail Varshavski, DO) who, in another useful (and easy to watch) conversation,
https://youtu.be/XVjLT3pinW0
point out that it’s not wrong to be skeptical and question data. While reviewing the science and the scientific method, they discuss the harm from tribalism and politicization. Also, at 59 minutes, there’s an explanation about how the variants arise.
However, the skeptics are wrong to dismiss all data from formal regulatory and research sources. The scientific literature is best evaluated over time and in proportion with the number of supporting reports. As in the case of the Wuhan doctors who stood against their government to call the world’s attention to the outbreak in the first place, minority reports should be considered. The valid reports will stand the test of time, public scrutiny, and real world observation. In contrast, as in the case of the (infamous) retracted papers in Lancet and JAMA, questionable data will be disproven.
If we can’t agree on the above paragraph, there’s no common ground for discussion.
As for the questions I often receive about my personal sources (in reality, my integrity): I use as many sites as possible. I certainly do not refer to only one silo of information. And, yes, I have watched all of the videos people share – at least until last night, when my friend linked to ten. I have worked through over half of them, and watched the first part of all of those.
I prefer to evaluate the myths themselves, rarely discussing the validity of the sources, except to point out those falsehoods or to point out obvious pre-existing biases based on the statements of the speakers themselves.
For instance, there are repeated referrals to Robert F Kennedy, Jr., who isn’t a good source. He has made inaccurate claims about vaccines for years, shifting from blaming measles vaccines to aluminum and mercury & he makes money from his anti-vaccine advocacy.
The doctor at the school board meeting loses validity right from the first by flatly stating that masks cannot protect from any virus. Surgical masks and N95s work. https://www.aerzteblatt.de/int/archive/article/217467
He repeatedly talks about “the vaccine,” when there are at least four, developed by different companies, tested in different sites. Are all the nurses and other personnel involved going along with some conspiracy(ies) promulgated by corrupt doctors and companies?
He is absolutely mistaken about enhancement by the vaccines – as Dr. Zubin Damania pointed out in the first video above, real world observation on the sheer numbers of vaccinated disprove this myth.
The event he referenced about in Barnstable, Massachusetts is an anomaly, due to large indoor gatherings.
https://www.cdc.gov/mmwr/volumes/70/wr/mm7031e2.htm
The pdf of the actual report is here https://www.cdc.gov/mmwr/volumes/70/wr/pdfs/mm7031e2-H.pdf
In fact, Barnstable answers the doctor’s question about why we’re seeing a surge in summer: people who were previously “socially distanced” are now gathering with fewer precautions. (Add the fact that the biggest breakouts are occurring in areas where close spaces and air conditioning are predominant.)
In the rest of the world, the vaccinated are less likely to get infected at all. At least 1/3 less likely, perhaps closer to 90%.
(This is pre-peer-reviewed data.)
https://spiral.imperial.ac.uk/handle/10044/1/90800
https://www.medrxiv.org/content/10.1101/2021.06.28.21259420v2?ijkey=43686632fd3918a950438cfefd8a2fc06e73b0ac&keytype2=tf_ipsecsha
In one video recommended, Geert Vanden Bossche, DMV, PhD, who is a frequently referred to, emphatically states that there is a virus, that it is highly infectious and it is deadly and that the vaccines are “excellent” & prevent disease – meaning the severe effects of infection. However, since they do prevent infection, I believe he is wrong about using vaccines in the middle of the pandemic.
The largest number of people becoming infected, and by corollary, becoming infectious, symptomatic, requiring hospitalization and dying, are unvaccinated. What we are seeing is that the vaccinated who do get infected are less sick – even though they are older and have more comorbidities.
There may be a kernel of truth in what Bossche says (in spite of the decreased numbers infected), since the vaccines were authorized first for the elderly and sick, who were also most likely to have an incomplete immune response.
Vanden Bossche proposes that the variants come from patients with partial immunity in the same way that antibiotic resistance occurs when bacteria are exposed to antibiotics in already infected patients. As pointed out in the Dr Z and Dr. Mike explanation about how viruses mutate, the variants occur after thousands or millions of replications in infected people. The viruses first have to infect, then they have to survive and be infectious.
The vaccinated are much less likely to get infected in the first place so the numbers of infections that are necessary to happen for the event of mutations and spread to others occur in the unvaccinated. So fewer infections mean less chances to mutate.
Vanden Bossche doesn’t answer the question: “What do we do?” The alternative was to let them get sick and risk death, a risk which is much greater in this population than in younger people who likely have a stronger immune response.
Mike Yeadon, Ph.D. is another “expert ” that is frequently referenced because he once was a head researcher and CEO at Pfizer. He was one members of the team that did early mRNA vaccine research. Even he notes that he repeats that government shouldn’t be trusted. Included in contradictory statements, he claims that there’s no virus, after saying older and sicker people should probably choose to be vaccinated. What infection is Bossche talking about if Yeadon is right?
There’s an emotional video at the “A Warrior” vlog that has too many distractions to be useful in fighting for sane policy, with its emphasis on 9-11 and pedophile truthers. But I’ll cover some of the obvious errors:
Dr Sam Smith is wrong about the SARS-1 animal experiments. https://www.google.com/amp/s/mobile.reuters.com/article/amp/idUSKBN2A22UW
Il repeat: Do you believe that any group is powerful enough to suppress the observation of the effects of 500,000,000 doses of different vaccines all over the world – 350 million in the US, alone? – by the hundreds of thousands of doctors & even more nurses and other professionals who are involved and would need to be complicit?
Smith’s major objection is the regulation of treatments and what he believes is a politically motivated exaggerated risk of COVID. However, I know several people who have been hospitalized with the infection, and several friends have lost relatively young loved ones to it. I’m sure you have the same experience.
An August 26, 2021 “McCullough Report” podcast begins with a major myth: that there are 90% false positives in asymptomatic testing. That number might actually be 2-3% for saliva tests. But is closer to 1%. Confirmatory tests are recommended for any positive test.
https://pubmed.ncbi.nlm.nih.gov/34238663/
https://pubmed.ncbi.nlm.nih.gov/34223865/
https://pubmed.ncbi.nlm.nih.gov/34116245/
(McCullough does quote the correct percentage of hospitalized cases which are vaccinated in the UK and Israel: 40%. This number should be evaluated in relation to the percentageof vaccinatedin the community and who is getting sick. Both countries have a majority of elderly, who are likely to have less immunity efficacy, and were the first eligible for vaccination roll outs. These are also the people who are getting sick.)
BTW, going to integrity and trust, Zubin Damania has been active for years in fighting the politicization and socialization of medicine in the US, as have I. Google his conversations with Dr. Atlas, and two of the authors of the Great Barrington Declaration (which I also signed), Dr. Jay Bhattacharya and Dr. Sunetra Gupta. We are all secure in supporting vaccination, opposed to blanket lockdowns, draconian enforcement, and politicization of treatments by physicians.
Candace Owen’s rant
I usually agree with Candace, but this video that’s circulating is propaganda and over the top. I won’t embed the video but you can go waste 30 minutes if you want, at this Facebook page.
I listened to 27 minutes. She gets to employer’s around 20 minutes in.
She has some things right, others very wrong.
Right:
A. Yes, social media is wrong to censor doctors.
B. Yes, vaccines should be voluntary.
Wrong:
- She’s conflating an acute asthma attack with a prophylactic vaccine for healthy people.
- Where’s the evidence that the US government is even telling, much less pressuring private employers? (*That* would be “communism,” or socialism, if government controls business.)
- There’s approval by the FDA. It’s emergency approval, but approval, just the same.
- Well over half of the US – 55% – has had at least one shot. 49% fully vaccinated over the age of 12. 59% of those over the age of 18. 200 million people in the US alone is a significant trial. We’re way beyond the “experimental” stage, with millions of life-years of evidence.
- And, for my British Virgin Island friends, The BVI isn’t the US.
Now, as to the employers…
Do business owners have no say in who they employ or the conditions of employment? Does the government own the business, so can make company policy? Do business owners answer to customers or their employees?
I don’t agree with mandatory vaccination if government does the forcing. And employers should use their policies wisely and carefully, only requiring legal, safe, and ethical acts from their employees.
The vaccine is legal, safe, and ethical.
Unlike government mandates, a business owner doesn’t use threats of guns and prisons. He sets company policy. If employees don’t like it, they aren’t slaves or indentured servants who must stay & follow the rules. They can leave.
No one owns their job. No one owes them a job.
Arguments?
Debunking COVID Vaccine myths (mRNA)
Vaccines work to decrease infection &/or severity of infection. All vaccines have failure rates, dependent on the immune status of the patient and the mutations of the virus or bacteria.
Half of the Covid vaccines types used in the US (Moderna & Pfizer) are MRNA vaccines that stimulate production of an antigen protein for a short period, certainly not in every cell in the body, nor do they cause the disease or induce even a mild form of the disease – as the measles, smallpox, and the oral polio vaccines do.
Most current vaccines use either an attenuated virus, a killed virus, or an antigen protein produced by recombinant DNA in bacteria or yeast. These last have never been part of a virus or bacteria. And, in fact, recombinant DNA is used to produce the human insulin to treat diabetes.
The mRNA in the Maderna & Pfizer Covid vaccines aren’t continously replicated by the vaccinated person and isn’t incorporated into the DNA. They are present in the human body about 2-3 days, mostly in the local muscle tissue and lymph system, with some in the spleen, more rarely in the liver.
Yes, you more than likely had an attenuated form of those infections when you were vaccinated. Current measles vaccines can cause infection that can be spread to immune compromised contacts. One way polio was all but eradicated was because people who came into contact with the babies who received the oral vaccine feces would also be infected – effectively receiving a booster unknowingly. We stopped using the oral polio vaccine in the 90s because 1 in 20 million children got a polio like disease after the 1st ( only the 1st) dose. We warn families to avoid contact with immune compromised people for a time after a child gets the measles vaccine.
The process was used years ago in the vaccine against ebola, so there’s history for use in humans.
For more, https://www.ema.europa.eu/en/news/ema-recommends-covid-19-vaccine-moderna-authorisation-eu
Newly created artificial wombs in mice raise concerns among abortion supporters
Shouldn’t everyone should be concerned that anyone could object to saving the life of a human, at any stage of life? How telling that the major concern here seems to be. “Any unborn child could be considered to have a right to life”.
The eugenic and social implications go further than the right to life, alone, according to thid op-ed from the UK Guardian,
“”Many tech and media companies, including Apple, Google, Facebook, VICE and Buzzfeed, already offer to cover the cost of freezing their employees’ eggs so they don’t have to worry about dwindling fertility during the most productive years for their careers. Gestating a baby in an artificial womb may one day be a choice open to elite women whose companies will pay for it, or who can afford to cover the cost themselves. “Natural” pregnancy could be seen as a sign of poverty, of unplanned pregnancy, or a chaotic lifestyle.””
I sincerely doubt that there would be a stigma attached to natural, in utero, gestation. Couldn’t the decision to gestate be seen as a mark of wealth and leisure? Or rebellion against technology as breast feeding and natural birth were, back in the mid- to late- 1900’s?
Science fiction authors have addressed these issues. Yes, there are potential ethics problems in any future technology that allows human gestation outside of the mother’s body. However, validation of the right to life should not be a “concern.”
Normal & reality: a proposed definition for discussion
On one of the Facebook groups I follow, the conversation about the recent Arkansas law protecting conscience was diverted from the law itself by a sensational headline that reflected only the worst accusations of opponents & the reactions of group members to that headline.
During the conversation, I was questioned about my use of the term “normal” for healthy bodily functions. At the least, “normal” is that which doesn’t itself injure tissues & organs and doesn’t require technological intervention to produce or to prevent morbidity & mortality.
We are hearing & reading about demands that legitimate research results should be suppressed, watching physicians and scientists who express heterodox opinions be censored. Then we’re told that there’s a “consensus,” since none of the “objectionable” research is published, much less popularized, and the outliers are demonetized and covered with warning boxes.
Science isn’t a “consensus.” In science, true hypotheses are testable, with valid results capable of being confirmed by different observers under similar conditions in different labs.
That’s also a good definition of reality or “normal.” One that could be applicable to medical subjects like COVID or vaccines, as well as social and legal matters.
We’re being manipulated for reasons that have nothing to do with actual health, physical or mental. I can’t fathom a reasonable explanation. It looks like an exertion of power – social, financial, then legal.
Patients won’t be helped at all by forcing moral injury by requiring medical professionals to act against their conscience and we all lose when rational discussion is suppressed in the public sphere.
Healing Spinal Cord Injuries By Reprogramming Cells | Worldhealth.net Anti-Aging News
“[W]e may not need to transplant cells from the outside.”
Good news from Texas medical researchers!
It appears that specific stimulating factors may prove more useful in harnessing the body’s own ability to heal and regenerate than stem cells, whether from my the patient or someone else. This research into regeneration of nerve cells mirrors the use of epogen and nupogen long used to induce blood cell production.
https://www.worldhealth.net/news/healing-spinal-cord-injuries-reprogramming-cells
EDITED TO ADD:
Here’s a longer online article from “EurekaAlert!,” from the American Assocation for the Advancement of Science, publishers of the journal, Science.
South Africa COVID Variant and the AstraZeneca Vaccine
CNN & NYT coverage of events in South Africa concerning the AstraZeneca vaccine that’s being given in the British Virgin Islands are very poor.
The new study doesn’t come out until today, so the “news” reports are based only on press releases.
ONE variant. ONE country.
And the actual data isn’t even available yet, even as preliminary information…
From what is available information in these reports about South Africa: About 1500 young people, average age 31, were studied in South Africa, half received the vaccine, half a placebo. This study only evaluated one strain, and only mild to moderate infections, because this age group doesn’t tend to get sick.
All we really know is that in the South Africa study, similar numbers became infected with that particular strain and the serum from their blood didn’t do a good job of neutralizing that strain in the lab.
From the BBC news reports:
“Data from the Oxford-AstraZeneca vaccine team suggests their vaccine protects just as well against the new UK variant, but offers less protection against the South Africa variant – although it should still protect against severe Covid-19 illness.”
The vaccine *does* have high efficacy protection for the older strains & the UK variant. Not only that, but if vaccinated, the infectious period is shorter for these varieties.
There’s evidently no safety concern about the AstraZeneca vaccine from either study.
Beverly B Nuckols, MD
Jordan B Peterson makes a mistake (Times article)
Dr. Jordan B Peterson has a new blog up in response to the publication of a hit piece disguised as an interview in the UK’s Sunday Times.
I’m a big fan of Peterson, as is my husband. I first noticed his online videos of his college lectures on philosophy & psychology, then became aware of his activism and, finally, his “Rules for Life” which became the base of his book of the same name. Larry and I were lucky enough to attend Dr. Peterson’s conversation with Sam Harris, moderated by Douglas Murray, in London a couple of years ago.
The Times‘ recent published interview is even worse than Peterson describes, with gratuitous remarks about toxic masculinity & unflattering, skewed and unexplicable comparisons to Donald Trump.
He’s posted the audio of the entire unedited interview on YouTube and has links in this blog post to the article published 31 January, 2021.
Here are a few of the hostile remarks by the author, Decca Aitkenson, from that article:
“I don’t know if this is a story about drug dependency, or doctors, or Peterson family dynamics — or a parable about toxic masculinity. Whatever else it is, it’s very strange.”
…
“After 80 minutes on Zoom, the one thing of which I’m certain is that, were I as close to death as she assures me her father repeatedly was, this is not the person I would entrust with saving my life.”
…
“The more he talks, though, the more I wonder whether toxic masculinity might have been a culprit, too. His family history of depression might tell us something about the price to be paid for his bootstrap philosophy; that when life became excruciatingly stressful, Peterson’s stand up, man up, suck it up mentality didn’t work.”
And, finally,
“Parallels with Donald Trump come to mind; another unhappy man closed off from his emotions, projecting strong man mythology while hunkered down in a bunker with his family against the world.”
If there’s anything I’m certain about Dr. Peterson it’s that he isn’t “closed off from his emotions.” Aitkenson is delusional or a biased liar. She’s no “reporter.”
Why Georgia matters
Even failed “progressive” actions by US legislators are rarely, if ever, reversed. Often, they enable broader progressive changes.

As I write this, it’s nine days after the 2020 election and we still don’t know who will be inaugurated as President of the United States. In spite of the precipitous “calling” of the election by the AP an other media for Joe Biden, the actual result is not a given due to close votes in several States. Lawsuits and recounts will likely play out at least until the day of the Electoral College vote, December 14, 2020, if not beyond.
Georgia officials have announced that they will conduct a recount and audit of the vote in that State because the difference in the Presidential election votes is about 0.2%. There’s a chance that the State will determine who will be sworn in on January 20, 2021.
But the biggest impact for the State may be as a result of another election. (Or, technically, two elections.)
On January 5, 2021, the State of Georgia will hold a run off election to determine both of their Senators. Currently, it appears that both races can be handily won by the Republicans if they turn out as they did on November 3, 2020.

(Each race had several candidates and Georgia requires a majority to win. Republican John Purdue beat Democrat Jon Ossof 49.7% to 48%.

While Republican Kelly Loeffler only received 25.9% of the vote in the Special Election compared to the 39.2% won by Democrat Raphael Warnock, the other Republicans in the race bled off Loeffler’s votes have endorsed her, including Doug Collins, who had 19.9% of the vote.)
In the event that Joe Biden wins the Presidential election each of us, regardless of Party affiliation, should ask ourselves whether the current crop of Democrats can govern without turning our Nation over to the chaos that is the status quo in many of the cities they already govern.
In addition, it’s imperative to remember the consequences of compromises and the influence of the Left on policies of the future.
Take an example from my profession: 1993’s “HillaryCare” debacle. Hillary Clinton’s plan to centralize health care to impose universal, single-payer government financed health insurance failed due to closed door meetings and a chaotic lack of political planning. It still resulted in SCHIP, HIPAA, the Balanced Budget Act of 1997 that removed all privacy from medical records and forced utilization of mid-level medical personnel as employees of “providers,” the ridiculous idea that cutting numbers of physicians by restrictions on funding for residencies would save money for Medicare, and ultimately, ObamaCare.
The Republicans have already won 50 seats, at least, but that is no majority and ties would be settled by the vote of the “President of the Senate,” the Vice President of the United States. In the event that Biden is the final winner of the Presidency, those ties would go to Kamala Harris – or her VP after Joe resigns or is unseated.
It’s a cliché that we’re likely to hear slot in the next 2 months, but do keep Georgia on your mind.
Scott Atlas, MD, in his own words
You’ve probably heard about the new doctor, Scott Atlas, MD who is advising President Trump on health policy during the last couple of months.
Here’s a video in which he describes his views and recommfations. You might be surprised!
Dueling Statements by “Experts:” More COVID-19 politics
On Blame
Amid sanctimonious reassurance that they don’t wish bad things on the President – or his “cronies” – Facebook, Twitter, and, certainly, the media are claiming that the President is responsible for each and everyone of the US deaths due to COVID-19.
(I won’t link to the sites, giving them more traffic. It’s easy to find samples.)
What would you have done? Scare tactics? Usurp State & local government with Federal force?
How would you shut down the economy and our kids’ education even more severely without imposing martial law, forbidding even “mostly peaceful” protests, using military guns to enforce your edicts?
The people getting sick aren’t just “Trumpsters” running around in MAGA hats at the White House.
In fact, most cases are nursing home patients and household contacts, people who necessarily live together.
And just as many, if not more, have died of suicide, overdoses and homicide – in addition to the increase of deaths due to heart attacks, strokes, and Alzheimer’s because of the lockdowns and lost jobs and businesses.
From Milwaukee, “[D]eath tolls would amount to 514 overdoses, 455 COVID-19 deaths, 193 homicides, and 120 suicides.”
And, no, the President hasn’t “lied” about the serious nature of the virus. In my opinion, he has chosen to give the best case, rather than worst case scenario whenever possible.
About the “Born-Alive” Debate
For those interested in the Born Alive issue, here’s a “pro-choice” leaning “FactCheck.org” article that generally has the details right. It’s the conclusion that is flawed.
We don’t know the specifics of President Trump’s Executive Order, but there’s quite a bit of controversy in social media and the news media.
The Fact Check article claims that neither the 2002 Act nor the 2019 (failed) Bill are necessary due to homicide laws in the States as well as Federal law.
However, there has always been a very real debate about both the babies on the cusp of viability and babies born alive in the process of an induced abortion.
The latter was addressed in the 2019 Bill that failed to pass. Specifically, that Bill (would have) mandated standard of care medical attention.
A modest proposal for COVID-19 response (Or, I’m not King, but)

JAMA table 1, comparing efficacy of masks
If I were in charge of the public health response to COVID-19, I would implement the following:
Pharmacy Boards should never get between a doctor and patient except in matters of life and death or illegal practice. Politicians, State Medical Boards and our House of Medicine professional organizations should defend our legal practice of medicine rather than threatening physicians and changing the rules during a pandemic.
2. Encourage shared information & fact-checking among physicians as part of our missions of education & transparency.
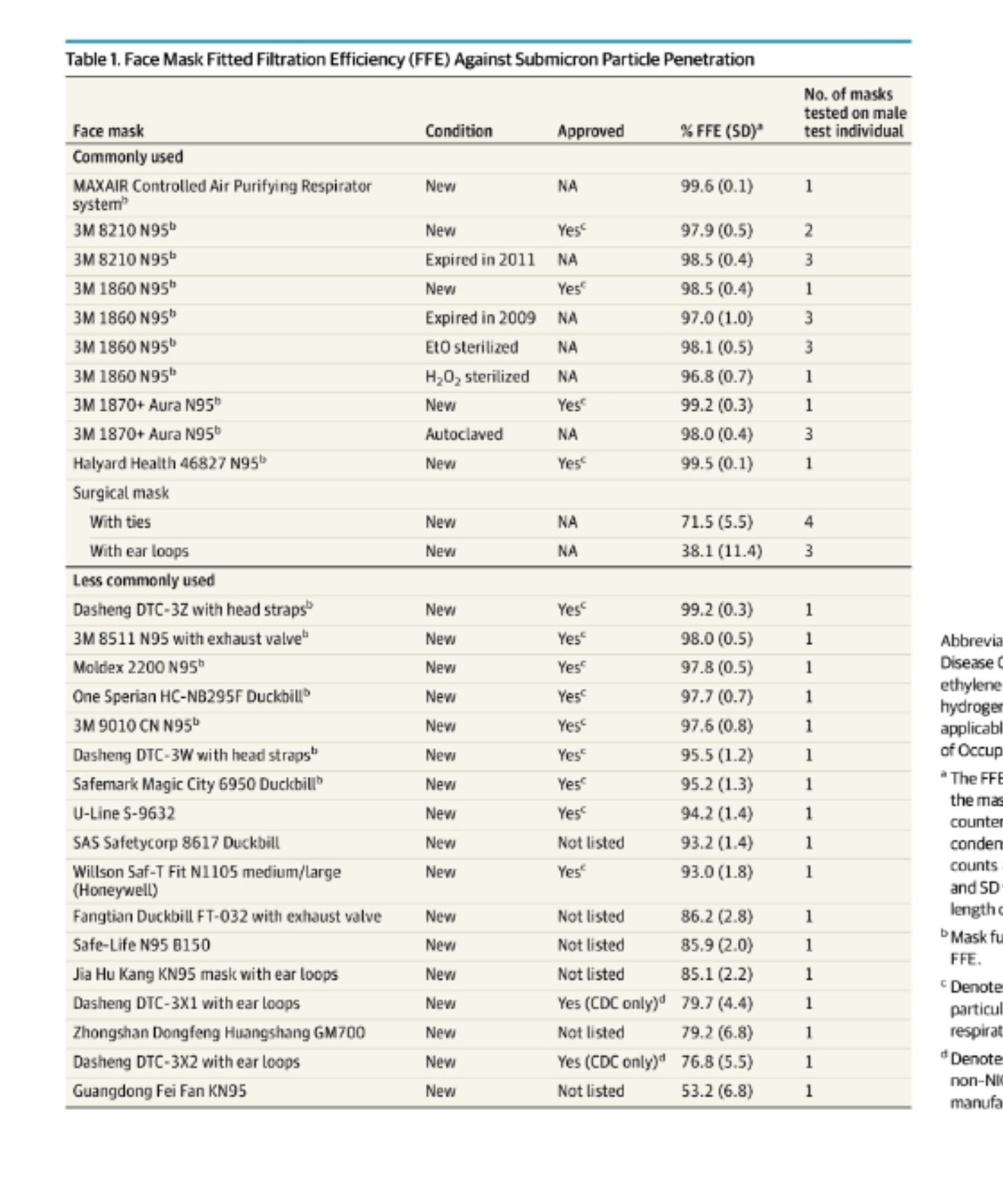
JAMA review of masks, August 2020
4. Where a high percentage of the local population tests positive, local authorities should consider – and have the ethical responsibility to – impose higher isolation measures like masks and public distancing. The threshold for mandates must be locally determined with public input, and explained – clearly, frequently.
This means you, anti-maskers!
5. Stress that surgical procedure masks are nearly as effective as N95 masks, blocking nearly as much aerosols and viral particles for both wearer and those around us. Medical providers and those with a high risk of prolonged close contact need fitted N95 masks, the rest of us don’t.
Single layer cut-up T-shirts and homemade masks, balaclavas or bandannas, aren’t very effective protection at all, either for the wearer or the people around us. N95 Masks with single valves are a money-maker, but not nearly as effective as surgical masks, even with an added filter layer.
8. Begin early prophylaxis with hydroxychloroquine/zinc and/or inhaled steroids for the willing & likely exposed.
REFERENCES
Treatment dosing (always allowing treating physicians who prescribe determine need & frequency of alternate doses & monitoring)
This isn’t a prescription!
Hydroxychloroquine: 400 mg. twice on day one then 200 mg. twice a day for either 5 or 10 days;
Azithromycin: 250 mg. tablet, 2 on day one, 1 on day 2 to 5;
Budesonide: unit dose via hand held inhaler or nebulizer twice a day. (I’m looking for references for this one. )
Zinc 150 mg. to 250 mg. a day indefinitely. (Best evidence for lozenges or syrup multiple times a day. See references.)
Vitamin D, 1000 IU a day, up to 4000 IU is safe
Vitamin C, No set dose, but extra will be excreted in the urine or feces, can cause diarrhea.
References
Journal of the American Medical Association review. Published August 11, 2020. (Free, with Tables)
CDC recommendation on cloth masks:
https://wwwnc.cdc.gov/eid/article/26/10/20-0948_article
John’s Hopkins recommendation:
Zinc:
https://www.uchealth.org/today/zinc-could-help-diminish-extent-of-covid-19/
Journal article on treatment for the common cold: https://www.acpjournals.org/doi/10.7326/0003-4819-125-2-199607150-00001
Hydroxychloroquine/azithromycin protocols
International Journal of Infectious Diseases (Henry Ford or Ashad report):
https://www.ijidonline.com/article/S1201-9712(20)30534-8/fulltext
https://www.ijidonline.com/article/S1201-9712(20)30600-7/fulltext
On synergistic effect of hydroxychloroquine plus steroids:
https://www.ijidonline.com/article/S1201-9712(20)30613-5/fulltext
Budesonide
Description of study in progress on treatment for loss of smell in patients without severe symptoms:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7370627/
Vitamin C safety:
Note: comments are off. Please comment on my Facebook page, Beverly Nuckols.
Edited 31/08/20 12:30 for mis-spellchecked word. BBN
Consult this (Dr.) Atlas

Dr. Scott W. Atlas, former Chief of Neuroradiology at Stanford University Medical Center, current Senior Fellow at Stanford’s Hoover Institute, author, and public health policy consultant was added to the White House COVID-19 task force this week. Unfortunately, he and his appointment have already become a political target by some.
Far from being unqualified, or someone who “clearly wouldn’t know science if it kicked him in the atlas” (see above link – I refuse to give clicks to the original source or the ignorant woman who spoke those words), Dr. Atlas speaks common sense, science-based truth, as in this video from 23 June, 2020 interview with Peter Robinson of the Hoover Institute’s. “Uncommon Knowledge.”
In fact, Dr. Atlas states what I’ve been saying since I heard about the virus outbreak in Italy, while attending Carnivale parades just a few miles away in

Carnivale float, Nice France, depicting Chinese labor in Fashion industry.
Nice, France: the reaction by governments and fearful people has been just as bad if not worse than the results of the infection itself.
The initial lockdown was correct, but we have new data – and new models – every day. Yet, we are still acting as though the early models were accurate.
Worse, instead of “flattening the curve,” the call is to conquer or eliminate the virus “at all costs.” The latter has never happened and will never happen with a Coronavirus. There is the possible exception of the elimination of smallpox, a much more deadly disease, at the cost of egregious human rights violations and even deaths.
I’m surprised that anyone would attack Dr. Atlas or his qualifications. Before you dismiss him, please listen to his testimony and critique the facts rather than the source.
Interview with Dr. Immanuel
14 minute interview with Houston TV reporter.
She’s a warrior, all right! Worth your time!
I would like to see some data, but lots of other doctors report the same results, and I’d like to see some of their patient information, too. (Ages, other meds, vitals, timing, symptoms.)
She does say wear a mask if you can’t be on prophylaxis and to make other people comfortable. I would call her regimen a “treatment” rather than a “cure.”
But the biggest fuss has been about Dr. Immanuel’s religious beliefs. I’ve heard Baptist, Assembly of God, even Church of Christ preachers say much the same about the hidden powers in the world. Maybe not the origins, but their existence and, as Jesus Himself said, the need for prayer and fasting to deal with them.
I’ve been told that her religious views are a distraction and counter-productive for the Medical issues and “science.” But Dr. Immanuel doesn’t even bring up her religion until she’s questioned in this interview and didn’t bring it up at all in DC.
The detractors don’t understand the cultural background and how many Christians – across the spectrum from those who believe in the indwelling of the Holy Spirit to those who only remember the story of St. Michael – will recognize the theme.
Dr. Stella Immanuel and political eugenics
Were you triggered by the religious views of Nigerian born and trained, Texas licensed and practicing, Dr. Stella Immanuel?
(As of Midnight, 30 July, the video was available at https://www.bitchute.com/video/09K3kIwzeewO/?fbclid=IwAnR2E-LChNhpqOktcV4GPeT0ZS79cdf1tjdlnfNSlpGNWMCW6vVYYnHLCbjU so I was able to watch the rest of the docs.I am impressed especially by Dr. Joseph Ladapo, beginning at minute 33.)
COVID-19 Treatment – Analysis of 65 global studies showing high effectiveness for early treatment
https://c19study.com/?fbclid=IwAR2QTfcqe3nlW81BG8rE7pgxyUMgMlcPC2J7Un3xDTT2mqsazlHTzJurpFc
39 of the studies were peer-reviewed.
43% of COVID- 19 deaths linked to nursing homes
“”You had this political conspiracy theory that the deaths in nursing homes were preventable,” said Mr. Cuomo.””
At a press conference today, New York Governor Andrew Cuomo insisted that his March order requiring NH’s to accept COVID positive patients from the hospital didn’t cause deaths – in spite of the fact that it’s estimated that those orders caused more than 6300 such transfers.

Click to view the percentage of death in NH by State
NY didn’t mandate NH testing until mid-May. NJ required testing by May 26th!
Right to Life, COVID, 16 May, 2020
The “Right to Life” means the negative right not to be killed by intentional acts. It’s not the right to force others to invest our life, liberty or property other than the duty to intervene against infringement. This is a basic negative right, not a positive right.
There’s a huge difference between personal responsibility in avoiding a risk to yourself and actively causing harm to someone else. Self-defense rather than selfish demands, using only appropriate force on others.
You know, the old “your right to swing your fist ends at my nose!” (Especially Appropriate in this case.)
*You* take the actions *you* believe are responsible. Only frequent places/businesses that require masks if you want, do the work necessary to maintain the social distancing you are comfortable with. Don’t force everyone else to do your work for you.
Test the story! (COVID-19 Fake News)
Right at the top of the page is this disclaimer: “”Anyone can publish on Medium per our Policies, but we don’t fact-check every story. For more info about the coronavirus, see cdc.gov.'” Good advice.
#BVILove, #Coronavirus Delayed, not “beaten.” (One small country’s COVID-19 story)
Here in the small Nation of the British Virgin Islands, we’ve delayed, but we haven’t “beaten,” or completely avoided, the disease caused by the novel, or new, Coronavirus, COVID-19. Everyone who hasn’t yet been infected is still at risk. A lot of us will eventually catch the virus if and when we once again interact with the world at all.

If you want to learn about the current state of the science, this video is excellent by a fantastic teacher.
The Nation has done an excellent job of blunting the effect of the disease, beginning with closing all ports of entry to everyone except residents, back in March, followed by a 6 day “lockdown” with an in-home curfew at night and limitedbusiness and shopping.
Beginning about April 2, Government began enforcing a 24 hour in-home curfew, shutting business and forbidding residents from leaving our homes.
There have been 5 people with positive tests. 4 of them caught the disease in other countries and one person may have caught the disease from the last of those 4. The first 3 had mild cases and appear to be recovering.
Unfortunately, that last case was a woman whose disease was only discovered when she became very sick and had to be admitted to the hospital. She died the next day. One of her contacts has tested positive, but has mild symptoms. Unfortunately, not all of the people she might have interacted with have been identified and tested.
Hopefully, over the last 6 weeks, the BVI health department has had time to plan and prepare for multiple sick patients.
Even more: I hope that researchers around the world will come up with good treatments and discover why some patients get so sick so fast.
If there’s ever a vaccine, it’s years away There haven’t been any successful vaccines for other human strains of coronavirus.
It appears from some recent random testing in the US, that about 25% – 30% of an exposed population contracts the disease. Most either have no symptoms or mild symptoms. A small minority gets sick enough to be hospitalized, and a fraction of those end up in the ICU.
You may have heard about the high “case fatality rate,” reported anywhere from 0.01 to 10. Remember that this statistic only counts those who have been tested, predominantly those sick enough to be admitted to the hospital.
There is good news in addition to the fact that most infected people have mild or no symptoms: evidence that we have immunity after recovery comes from one of the treatments undergoing research: serum containing antibodies from the blood of recovered patients helps other people get well.
The scary part of the story is that the virus is very contagious, largely because people without symptoms can spread the disease. Medical personnel have been surprised by what appears to be the unprecedented, rapidity of the onset of Acute Respiratory Distress Syndrome (ARDS) in some patients, usually about day 12 to 14 of the symptoms. In a matter of a few hours, patients become very short of breath, requiring intubation. 80%- 90% of those intubated have died in the ICU.
The virus can also cause the body to produce proteins causing increased coagulation (the tendency for blood to clot). It also can directly infect the heart muscle and brain.
As our country opens up, and goes back to (relatively) more normal interaction, it’s important to remember that infected people may not have symptoms, but are still able to share the virus and spread the disease. They don’t know they have it and you certainly can’t tell by looking at them.
We will probably see our neighbors continue “social distancing” and wearing face masks when we leave our homes. And yes, inevitably, some of us will get sick.
Front lines in the ICU with COVID-19
Reality is teaching a hard reality lesson with COVID-19.
This video concerns the minority of COVID-19 patients who require intensive care and the less than 1 percent who die of the disease. The discussion about the course of the disease and treatment is possibly too technical and brutal for the general public, so watch the whole thing with care.
However, I’m hoping to spur conversations about end of life in light of the broader COVID-19 crisis and specific crisis events.
This is a tough, highly technical discussion between Dr. Zubin Damania, a blogger otherwise known as “ZDoggMD” and Barbara McClean, MN, RN, CCRN, NP-PC, an expert in Critical Care & Intensive Care medicine in an Atlanta, Georgia teaching hospital with over 100 ICU beds. The first few minutes show Barbara McClean as a compassionate caring practitioner and educator. I believe and trust what she says about the worst case (stressing, again: fortunately these are the minority!) outcomes with COVID-19.
If you want to get to the meat of the video, there’s a “philosophical discussion” about the very real, unique in this modern age, futility of CPR in COVID-19 patients whose hearts stop due to the disease at 35:00 to 41:00.
There’s also interesting information about Personal Protective Equipment (PPE) difficulty (not shortage, but the physical reality) at the segment 30:00 to 35:00 minutes.
COVID-19 is, as Ms. McLean says, an unpredictable, sometimes deadly disease. Currently, patients can go from minor symptoms to death due to respiratory failure and cardiac arrest in as little as 4 hours. There is very little success to date in attempts to resuscitate patients who “code,” whose hearts stop, while in distress due to the virus.
I can’t stress enough that we need to talk, we need to make decisions among our families and to understand that this disease takes some options, some autonomy we have come to assume are our rightful “choices,” completely off the table. This disease doesn’t care what we want.
I’m unable to turn comments back on for this post. Please post comments to my Facebook page and I will try to keep up with replies. Let’s keep this on the level of philosophy and medical ethics. I will delete political criticisms.
Let’s keep this on the level of philosophy and medical ethics. I will delete political criticisms.
People ‘shed’ coronavirus early, but most likely not infectious after recovery
A study of only 9 people, but it’s a start.
Essentially, you can spread the virus even when your symptoms are mild, but probably won’t after 8 days.
Don’t eat the COVID-19 (Coronavirus)
The good news is that we were warned and it’s Spring, not Winter. (And we don’t routinely greet acquaintances with real kisses in the US.)
The really good news is that you aren’t helpless.
Chances are, most of the people who get sick picked the germs up with their hands and put them in their mouth, nose or eyes. (Gross, I know, but, trust me, I’m a doctor and a mother. I can be more gross than that when I want to get your attention.)
I tend to be a skeptic about panics, and so much of the news coverage about coronavirus is political hyperbole, but … I’m reading some worrisome stories from doctors dealing with the outbreak of COVID-19 in Italy.
Don’t panic, and don’t share! The coronavirus is spread by particles, droplets that have to enter your body by way of your nose, mouth or eyes. While it’s possible that someone might infect you by sneezing or coughing in your face, most viral infections are spread because of poor personal hygiene.
Virtually no one is immune to this coronavirus and we won’t have a vaccine for months, so people are panicking. I’m not, and here are some reasons why:
The US isn’t Italy. For one thing, we have a younger population. And, although the Lombardy region in Italy is modern and advanced, we have a higher intensive care capacity.
After all, we easily absorb the burden of influenza: up to 49 million infections, half a million hospitalizations, and 50,000 deaths every year due to influenza and hardly anyone even notices.
And we’ve had more warning than they did.
Here’s how fast influenza spreads each year in the US. If we don’t practice excellent self- protection, it’s a preview of how fast COVID-19 could spread.

Confirmed hospitalization history for Influenza in the US. Red = 2019-20, Orange =2017-2018
What’s the rate of spread of influenza in the US each year? This year? The graph above shows the historic rates of confirmed hospitalizations in the US. The red line is this year and reflects just over 16,000 patients, so far. The bright orange at the top is 2017, when we had a poorly matched vaccine.
There have been 200,000+ positive influenza tests reported to the CDC this year, 16,000 hospitalizations, and 136 pediatric flu deaths – not elderly patients with chronic diseases – this year.
We call it “seasonal” influenza for a reason. People tend to share the virus more in winter because of Thanksgiving and Christmas gatherings (and travel) and because children are in school. Sharing germs.
The coronavirus cases in the US sometimes have unknown “patient 1,” but the bulk have all involved clusters of patients with known physical and/or close contact with someone who was sick. The deaths have mainly been patients in one nursing home and a (different) hospital. In these sites, sick people were exposed to the droplets much more than you or I might be, because medical treatment accidentally aerosolized secretions.
COVID-19 symptoms are a fever over 100.5, a dry cough, and, for some, rapid onset of trouble breathing. Ther might be a runny nose or diarrhea, but there isn’t vomiting.
Use common sense and easy-to-achieve precautions. Wash your hands, don’t touch your face (eyes, nose, mouth), stay out of crowds, kindly and gently use what influence you have to encourage others to do the same.
If you get a fever, don’t go to the ER unless you are having trouble breathing. Call your doctor, and “self-quarantine.”
Most of all, Don’t share your germs and don’t pick up others’ viruses and put them in your body.
(Comments are closed. Please comment on my Facebook page.)
To kill or not to kill – or even to call it killing?
It seems that an advocate of Euthanasia and Assisted Suicide (EAS), which is legal in Canada since 2016, complained to the “The Protection of Conscience Project” administrators about their use of the word, “killing,” rather than “Medically Assisted Death” (MAD) when writing about the law. The wording of the objection exposes the potential limitations even on thoughts, much less the act of refusal, of physicians who object to participating in EAS.
(*EDITED An earlier version stated that licences were at risk. Not yet.
BBN 11 February 2020 12:30 AM)
More thoughts on Texas Advance Directive Act
I was asked about the #BabyTinslee case and what we should do, what can we do, in the disputed cases.
We need to educate more. People don’t understand basic medical ethics in this day of “choice.”
Autonomy doesn’t supersede nonmaleficience. In other words, the First Principle of medicine, “Cure when possible, but first do no harm,” always should guide us, rather than “wants” or “choice.”
In the end, doctors are the ones actually performing the acts and we’re most likely to understand the projected outcome. We benefit from oversight by colleagues and the community, both informally and in the process prescribed by the Texas Advance Directives Act.
Some people demand that every one of these cases go to court, for “due process” and “cross examination.”
But judges and courts can’t be as knowledgeable as doctors are. Their decisions are necessarily informed by dueling (paid) lawyers and (hired) medical experts.
In all the cases that have gone to court, the family has had quite a lot of notice, but the 48 hour notice before the committee meeting is perceived as too abrupt, especially since the relationships all appear to be adversarial by that point.
(And who could get your family to a meeting in 2 days?)
The 10 days isn’t thought to be long enough to arrange a transfer, either. Again, in many of the Court cases, the attempts to find another doctor willing to accept the patient’s care has begun before the committee meeting.
Doctors acknowledge the great trust and privileges we are given by agreeing not to abandon our patients. When we have a disagreement with a patient or surrogates (usually a familymember), we accept that we must continue treatment for a period of time. But not indefinitely.
If we could get the reforms that have been attempted to lengthen the statutory timeframe (multiple times) since before 2005, the TADA would be much better. It’s still the best process we have, currently.
Click here to get your “Choose Life” license plate

Rick Perry RickPAC
Yes, I'm still for Governor Perry!
RickPAC
SiteMeter
